
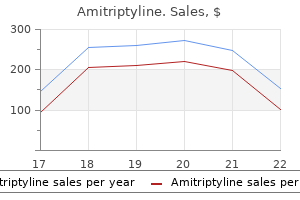
Amitriptyline dosages: 50 mg, 25 mg
Amitriptyline packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

25 mg amitriptyline buy free shipping
Modern humans probably originated from a small population residing in Africa that had been evolving over tens of millions of years mood disorder book 50 mg amitriptyline discount with mastercard. Within the previous 50 depression or grief test purchase 25 mg amitriptyline otc,000 years, members of this ancestral inhabitants migrated "out of Africa," settled the globe, and solely recently, over the previous 5000 to 10,000 years, multiplied exponentially. These rare genetic variants arose more lately from spontaneous mutation in the past 10 millennia, after the migration of many people out of Africa, and are typically observed occasionally (<0. Evolution influences the frequency of variants that have an effect on human phenotypes (such as endocrine diseases) via the method of pure choice. If a disease is no much less than mildly evolutionarily deleterious, then most common variants related to that disease will solely modestly increase disease threat. Finally, the number of genes that contribute to illness in a single particular person (mendelian or polygenic disease) might be associated to the strength of impact of anybody variant on disease danger. By definition, variants that cause mendelian disorders have robust effects, whereas variants contributing to danger of polygenic diseases will sometimes have more modest effects. Thus, most variants with robust effects on disease might be uncommon, particularly for those ailments that are clearly deleterious from an evolutionary standpoint (lethal earlier than reproductive age). Heritability describes the proportion of a disease/trait that can be explained by genetic components; the heritability of most endocrine ailments ranges between 20% and 80% (see Table 4-1). The demographic history of contemporary human populations explains the presence of frequent and rare genetic variants in the human genome (see Table 4-2). Common variants are largely historic, and sometimes have comparatively modest scientific results, whereas rare variants are inclined to have arisen extra recently and might exert larger medical results (Table 4-4). On the other end of the spectrum lie the so-called widespread illnesses, similar to sort 2 diabetes, characterized by (1) many variants in many genes (polygenic), (2) high frequency within the inhabitants (>1: 20), and (3) low penetrance (<1. Owing to their simple genetic architectures, mendelian endocrine issues were ideally suited to genetic mapping utilizing the methods of familial linkage mapping developed within the Eighties. For example, penetrance of mendelian variants could presumably be precisely estimated provided that these variants have been ascertained in the basic inhabitants, quite than in chosen households with a particular genetic background. Large-scale sequencing research within the common inhabitants, which can establish all variants, uncommon and common, are now enabling such estimates. Such studies have discovered that, when ascertained in the general inhabitants, the so-called mendelian variants are much less penetrant that was estimated from family-based studies. Thus, they can be applied to identify genetic elements underlying diseases occurring in a inhabitants of unrelated people. Unlike medical risk factors/ biomarkers affiliation studies, correlation in genetic association research implies causation as a result of genotype at all times precedes phenotype. Such studies yielded a number of widespread disease associations however have been poorly reproducible and confounded by false-positive outcomes arising from inhabitants stratification. As with the chromosomal linkage studies of the past; figuring out the causal variants/genes on a haplotype necessitates a combination of further affiliation evaluation (fine-mapping16,17) and functional experimentation in mannequin systems. While we distinguish between these two extremes of genetic structure, it is essential to appreciate that many problems lie between these two extremes: uncommon variants of average impact can have an effect on the common type of the disease, and genetic and nongenetic modifiers can strongly affect the result of mendelian problems. Furthermore, many polygenic endocrine disorders also have rare mendelian forms (see Table 4-1). The genes for a wide range of mendelian endocrine ailments have been mapped, revealing nice mechanistic perception. Although mendelian illnesses have offered priceless insights into pathophysiology, not all insights gained from mendelian types of illness translate on to the common types of disease. Thus, genetics of both mendelian types and common polygenic varieties could have necessary, usually complementary impacts on our understanding of illness and on affected person care. The sections that follow discuss consultant examples of mendelian and polygenic endocrine problems that illustrate necessary concepts in gene discovery, understanding of the impact of genetic variation on disease, and implications for clinical care and insights into new biology. We focus on a quantity of lessons of mendelian illnesses and spotlight three polygenic endocrine diseases/traits: (1) type 2 diabetes, (2) stature, and (3) serum lipids. At one end of the spectrum are mendelian ailments cause by few variants in few genes every with a large particular person effect on illness danger. On the opposite end of the spectrum are widespread illnesses and traits which would possibly be attributable to the combined effects of many variants, observed frequently within the inhabitants, each with a modest individual impact. Genome-wide association research for complicated traits: consensus, uncertainty and challenges. Mendelian Endocrine Diseases GeneticArchitecture Mendelian illnesses symbolize one excessive of a spectrum of potential genetic architectures. The alleles inflicting mendelian illnesses are found in a small number of genes, are usually rare (<1: 1000), are extremely penetrant, and observe easy patterns of dominant and recessive inheritance. They are considered monogenic in that a mutation in a single gene causes illness in a person or family. But as completely different families segregating the same mendelian illness are identified and the causal genetic variants mapped, genetic heterogeneity is often observed: different alleles in numerous genes could cause the identical illness. This phenomenon, variants in different genes inflicting the same illness, is termed locus heterogeneity. It is important to bear in mind that locus heterogeneity is intrinsically tied to the precision of disease definition. When contrasted with frequent polygenic diseases, mendelian disorders exhibit relatively much less locus heterogeneity. In other words, an considerable fraction of mendelian illness circumstances may be largely defined by mutations in one or a few genes. Thus, much of the genetic architecture of mendelian ailments remains uncharted territory for genetic mapping. Modern sequencing applied sciences have facilitated a renaissance in mendelian illness gene mapping and will help enhance our understanding of the genetic basis of mendelian issues. DiseaseBiology Every endocrine organ ranging from the pituitary to adrenal is affected by well-described and less-described mendelian disorders. Mechanistic perception into illness biology has been gained from discovering the identities of the genes that lead to disease. When mutations in a selection of completely different genes can all trigger a disease (locus heterogeneity), further mechanistic insight into molecular pathophysiology becomes potential. This makes intuitive sense in the context of a molecular understanding of genes as encoding proteins that act in live performance to accomplish cellular capabilities. For other problems, a more complex picture emerges by which multiple molecular pathways are implicated. At the extent of a single gene/locus, genotype-phenotype correlations mapping allelic heterogeneity to phenotypic heterogeneity can provide detailed perception into how alterations in gene function have an effect on illness severity. Even when mutations of varying molecular severity are identified, they might not predictably have an effect on phenotype. The genetic causes of many mendelian problems stay unknown, however advances in sequencing technology have accelerated the pace of discovery.
Amitriptyline 25 mg generic fast delivery
Surgery was indicated because of a quickly progressing curve in a patient with a persistent potential for development tropical depression definition wikipedia amitriptyline 25 mg buy with mastercard. Supine bending films demonstrated a correction of the thoracolumbar curve to 15 levels (c) and of the thoracic curve to 20 levels (d) bipolar depression meds buy 50 mg amitriptyline fast delivery. We opted for a brief selective anterior fusion by a thoracoabdominal strategy due to the nonetheless versatile thoracic curve. Six years after surgery, the patient offered with a balanced spine and was symptom free (e). The radiographs show a superb curve correction with fusion of only two intervertebral discs (f, g). Idiopathic Scoliosis Chapter 23 625 In patients with small curves, men and women are about equally affected, but with increasing curve magnitude the female-to-male ratio adjustments to the drawback of feminine adolescents [6, 22, 23, 97]. The childish type (0 � three years) is extra frequent in males (3:2), and could additionally be associated with pathologic findings of the center, skull, hip, or psychological growth. However, some factors that seem to play a task in the etiology and pathogenesis of this spinal deformity have been detected. On the opposite, the circumferential development of the vertebral bodies and pedicles by membranous ossification was discovered to be slower than in controls. Asymmetrical anterior column progress with posterior tethering may result in scoliosis Genetic Factors Several research have proven that idiopathic scoliosis develops inside affected households with the next incidence than in the basic inhabitants [44, 233]. In one research, 27 % of the daughters of ladies with scoliosis (curves > 15�) were discovered to have scoliosis as nicely [84]. Studies with monozygous twins exhibited a concordance of almost three-quarters for the development of scoliosis whereas the concordance in heterozygous twins was discovered to be about one-third, which is still higher than in first-degree relatives [100]. Beside these observational approaches a quantity of attempts had been made to statistically analyze a possible linkage of genes to the disorder. However, such a gene has not been detected yet and the aforementioned research with monozygous twins recommend that variable gene expression and environmental elements additionally influence the event of scoliosis. There is a genetic predisposition for idiopathic scoliosis Connective Tissue and Skeletal Muscle Abnormalities Scoliosis is linked to several connective tissue diseases corresponding to Marfan syndrome. Therefore, alterations in the extracellular matrix of connective tissue have been the topic of investigations on the etiology of scoliosis. Changes in the paraspinal musculature had been also mentioned as possible etiologic factors. Several studies discovered a muscle fiber distribution (slow-twitch and fast-twitch) between the convex and the concave aspect of the curve [27, 189, 199, 201, 235]. However, it could only be speculated whether or not these alterations are the end result or the cause of the illness [129]. Connective tissue issues appear to play a task in scoliosis 626 Section Spinal Deformities and Malformations Thrombocyte Abnormalities, Calmodulin and Melatonin the myosin/actin contractile techniques of thrombocytes and skeletal muscle are fairly related. As thrombocytes are unbiased of the axial skeleton, changes must be impartial of secondary results caused by the deformity itself. Patients with larger idiopathic curves exhibited extra metallophilic thrombocytes, whereas the reticular sort was primarily found within the controls. This distinction was thought to be due to completely different membrane permeability indicating a membrane defect. Calmodulin interacts with actin and myosin and regulates the calcium influx from the sarcoplasmatic reticulum. It subsequently regulates the contractile properties of muscles and platelets and has also been investigated as a potential etiologic issue. Elevated calmodulin concentrations in thrombocytes had been discovered to be associated with progressive adolescent scoliosis while the degrees in sufferers with non-progressive curves and controls had been similar [102]. As melatonin binds to calmodulin and acts as an antagonist to it, it may additionally play an essential function within the regulation of the aforementioned platelet modifications. In conclusion, these reports recommend a defect within the contractile system of platelets associated with scoliosis. The rationale behind this classification is that progress of the backbone within the juvenile age (3 � 10 years) is somewhat regular [172] and that the pulmonary maturity reached after 5 years of age exhibits fewer cardiopulmonary risks [208]. The grownup idiopathic scoliosis has to be differentiated from:) major degenerative or "de novo" scoliosis (see Chapter 26) the adult idiopathic kind is an idiopathic scoliosis which already existed at the finish of progress and might exhibit progressive secondary degenerative modifications [1]. The classification relies on six different curve patterns, three lumbar backbone modifiers and a sagittal thoracic modifier. The curves within the scoliotic spine are differentiated into structural and non-structural curves. Two recent research have investigated validity and reliability evaluating the King and Lenke classifications [155, 182]. The Lenke classification considers all anatomical curve varieties and the sagittal thoracic profile Clinical Presentation History Patients presenting with idiopathic scoliosis before adulthood normally current with out severe clinical indicators and symptoms. Frequently, the scoliosis is accidentally discovered by family members, academics, friends, school nurse or family physicians because of the again or shoulder asymmetry. Teenagers sometimes realize the scoliosis is present when they have problems discovering completely fitting garments (waistline asymmetry). Severe pain, useful disability and neurological deficits are hardly ever current in adolescent idiopathic scoliosis and may immediate suspicion about. Several components are helpful in assessing the danger of progression [25, 125]:) menarchal status) breaking of the voice) beard growth) development spurt Investigations have proven that every one women have the menarche before the top of the expansion spurt and that no menstrual bleeding occurs before peak growth velocity. In boys, it was found that the expansion spurt is in its most intensive phase when voice breaking begins [80]. Adult idiopathic scoliosis usually presents with pain and/or incapacity because of:) secondary degenerative changes) sagittal or coronal imbalance Progression of adult scoliosis [1] could lead to growing waistline asymmetry and hip prominence and cause symptoms. The most common criticism is back ache due to side joint arthritis, disc degeneration or imbalance [93, 194]. Adult scoliosis could cause important ache and disability Assess danger factors for curve progression Physical Examination General Assessment Height (sitting and standing) and weight ought to be noted at every examination to monitor growth and establish a growth spurt. A full musculoskeletal assessment is indispensable to identify related pathology. Leg size discrepancies, limb asymmetries, arachnodactyly, foot deformities, foot size discrepancies (tethered cord) or basic laxity of the joints might point out secondary scoliosis. The pores and skin should be searched for:) hairy patches/dimples (spinal dysraphism)) caf�-au-lait spots (neurofibromatosis) e Perform a complete musculoskeletal exam Rule out secondary scoliosis by the use of a radical history and physical exam 630 Section Spinal Deformities and Malformations Curve Assessment Bending ahead is probably the most dependable scoliosis screening test Assess coronal balance In small curves not a lot may be seen when inspecting the again in the upright position. However, asymmetries similar to an S-shaped line of the spinal processes, a slightly more distinguished scapula or asymmetric lumbar triangles might point out the presence of scoliosis. When the curve is bigger, the deformity is clearly seen within the upright standing position. Side bending is necessary to evaluate the flexibleness of the curves and detect structural curves. Clinical curve evaluation should embody:) curve location (thoracic, thoracolumbar, lumbar)) convexity (right, left)) flexibility of the curves) extent of rib hump/lumbar bulge) shoulder level) pelvic obliquity) sagittal profile) sagittal balance) coronal steadiness the convexity of adolescent thoracic curves is totally on the best facet. Assessing the curve flexibility by passive aspect bending is indicative of the curve rigidity. The sagittal profile normally presents quite with a hypo-kyphosis/lordosis than with hyper-kyphosis/lordosis.
Diseases
- Acute necrotizing ulcerative gingivitis
- Brachydactyly long thumb type
- Short limbs abnormal face congenital heart disease
- Cutis verticis gyrata mental deficiency
- Histadelia
- Congenital generalized fibromatosis
Discount amitriptyline 25 mg otc
Similar changes in the disc result in herniation anxiety attack 25 mg amitriptyline purchase visa, inner disruption depression test k10 purchase amitriptyline 25 mg with mastercard, and resorption. Combined adjustments in posterior joint and disc can produce entrapment of a spinal nerve within the lateral recess and/or central stenosis. Changes at one stage typically lead, over a period of years, to multilevel spondylosis and/or stenosis. Spine 13(2):173 � 8 this meta-analysis relies on information from sixteen revealed stories. Macroscopic disc degeneration grades had been correlated with age, intercourse, and degree in 600 lumbar discs from 273 cadavers (0 � ninety six years of age). Male discs were considerably more degenerated than feminine discs within the second, and fifth to seventh life decades. Higher mechanical stress, perhaps mixed with longer dietary pathways, could additionally be liable for the sooner degeneration of male discs. Spine 27(23):2631 � 44 this paper offers a systematic semiquantitative evaluation of age-related morphologic modifications in the intervertebral disc and cartilaginous endplate which is based on 20 250 histologic variables. The study revealed important temporospatial variations with regard to presence and abundance of histologic disc alterations across ranges, regions, macroscopic degeneration grades and age groups. The detailed evaluation resulted in a practicable and dependable histologic classification system for lumbar discs which can serve as a morphologic reference framework. The article provides clear histologic proof for the detrimental impact of a diminished blood supply to the intervertebral disc that appears to initiate disc tissue breakdown starting within the first half of the second life decade. Spine 26(23):2543 � 49 Nucleus pulposus cells had been cultivated in a system where nutrient supply was depending on diffusion, subsequently simulating the situation within the intervertebral disc. It was found that the cell density was depending on nutrient provide and was inversely associated to disc thickness. Oxygen provide was not needed for cell viability however was wanted for proteoglycan manufacturing. Lack of glucose or low pH led to cell dying suggesting nutrient restrictions contribute to disc degeneration. Spine 21(4):415 � 20 Transport properties of solutes of various sizes and shapes have been correlated with the composition of the cartilage matrix. Increasing contents of proteoglycan, collagen or calcification resulted in higher restriction of solute motion. This finding confirmed that calcification of the cartilage endplate might need penalties for the nutrient supply to the disc and therefore for the onset of disc degeneration. A research relating lifetime exposures and magnetic resonance findings in identical twins. Spine 20(24):2601 � 12 Effects of lifetime publicity of 115 twin pairs to commonly suspected risk factors on disc degeneration had been assessed by magnetic resonance imaging and their affect was compared to age and familial aggregation, reflecting genetic and shared environmental influences. The outcomes of this examine suggested that disc degeneration could also be primarily defined by genetic influences, with environmental elements, extensively suspected of accelerating disc degeneration, solely having very modest effects. Spine 25(13):1625 � 36 It was investigated whether or not minor damage to a vertebral physique can lead to progressive disruption of the adjoining intervertebral disc. After cadaveric lumbar motion segments were subjected to complicated loading patterns to simulate typical actions, compressive damage to the bony endplates was noticed, altering the compressive stress distribution on the adjacent disc. Further loading cycles resulted in progressive structural modifications and deterioration of the adjoining discs. Adams P, Muir H (1976) Qualitative changes with age of proteoglycans of human lumbar discs. Bernick S, Cailliet R (1982) Vertebral end-plate adjustments with growing older of human vertebrae. Doita M, Kanatani T, Ozaki T, Matsui N, Kurosaka M, Yoshiya S (2001) Influence of macrophage infiltration of herniated disc tissue on the production of matrix metalloproteinases resulting in disc resorption. Friberg S, Hirsch C (1949) Anatomical and scientific research on lumbar disc degeneration. Fukuyama S, Nakamura T, Ikeda T, Takagi K (1995) the effect of mechanical stress on hypertrophy of the lumbar ligamentum flavum. Greg Anderson D, Li X, Tannoury T, Beck G, Balian G (2003) A fibronectin fragment stimulates intervertebral disc degeneration in vivo. Connect Tissue Res eight:101 � 119 Holm S, Nachemson A (1988) Nutrition of the intervertebral disc: acute results of cigarette smoking. J Gerontol A Biol Sci Med Sci fifty seven:M772 � 777 Iida T, Abumi K, Kotani Y, Kaneda K (2002) Effects of getting older and spinal degeneration on mechanical properties of lumbar supraspinous and interspinous ligaments. J Orthop Res 17: 829 � 835 Ito M, Abumi K, Takeda N, Satoh S, Hasegawa K, Kaneda K (1998) Pathologic features of spinal problems in sufferers treated with long-term hemodialysis. Spine 23:2127 � 2133 Itoi E, Tabata S (1992) Conservative treatment of rotator cuff tears. Spine 26:2550 � 2557 Johnstone B, Markopoulos M, Neame P, Caterson B (1993) Identification and characterization of glycanated and non-glycanated forms of biglycan and decorin in the human intervertebral disc. Biochem J 292(3):661 � 666 Jones G, White C, Sambrook P, Eisman J (1998) Allelic variation within the vitamin D receptor, life-style factors and lumbar spinal degenerative illness. Spine 27:78 � eighty three Kawaguchi Y, Kanamori M, Ishihara H, Ohmori K, Matsui H, Kimura T (2002) the association of lumbar disc illness with vitamin-D receptor gene polymorphism. J Bone Joint Surg Am 84-A:2022 � 2028 Kawaguchi Y, Osada R, Kanamori M, Ishihara H, Ohmori K, Matsui H, Kimura T (1999) Association between an aggrecan gene polymorphism and lumbar disc degeneration. J Bone Joint Surg Br 81:1058 � 1063 Kuno K, Kanada N, Nakashima E, Fujiki F, Ichimura F, Matsushima K (1997) Molecular cloning of a gene encoding a new sort of metalloproteinase-disintegrin household protein with thrombospondin motifs as an irritation associated gene. A histopathological investigation of intervertebral discs from 30 randomly selected autopsies. Spine 15:402 � 410 Matsui H, Kanamori M, Ishihara H, Yudoh K, Naruse Y, Tsuji H (1998) Familial predisposition for lumbar degenerative disc disease. Spine 23:1029 � 1034 Matsui H, Terahata N, Tsuji H, Hirano N, Naruse Y (1992) Familial predisposition and clustering for juvenile lumbar disc herniation. J Anat 198:three � 15 Melrose J, Roberts S, Smith S, Menage J, Ghosh P (2002) Increased nerve and blood vessel ingrowth associated with proteoglycan depletion in an ovine anular lesion mannequin of experimental disc degeneration. Spine 13:173 � 178 Miyamoto H, Saura R, Harada T, Doita M, Mizuno K (2000) the function of cyclooxygenase-2 and inflammatory cytokines in ache induction of herniated lumbar intervertebral disc. Kobe J Med Sci forty six:13 � 28 Murata Y, Onda A, Rydevik B, Takahashi I, Takahashi K, Olmarker K (2006) Changes in pain conduct and histologic modifications caused by utility of tumor necrosis factor-alpha to the dorsal root ganglion in rats. Immunohistologic markers for age-related modifications of human lumbar intervertebral discs. Okuda T, Baba I, Fujimoto Y, Tanaka N, Sumida T, Manabe H, Hayashi Y, Ochi M (2004) the pathology of ligamentum flavum in degenerative lumbar illness. Okuda T, Fujimoto Y, Tanaka N, Ishida O, Baba I, Ochi M (2005) Morphological changes of the ligamentum flavum as a explanation for nerve root compression. Panjabi M, Abumi K, Duranceau J, Oxland T (1989) Spinal stability and intersegmental muscle forces. Parkkola R, Rytokoski U, Kormano M (1993) Magnetic resonance imaging of the discs and trunk muscles in sufferers with persistent low again pain and wholesome control topics. Postacchini F, Bellocci M, Massobrio M (1984) Morphologic changes in annulus fibrosus during growing older. Roberts S, Menage J, Duance V, Wotton S, Ayad S (1991) 1991 Volvo Award in basic sciences.

Amitriptyline 25 mg generic with amex
Localization of vagal preganglionics that stimulate insulin and glucagon secretion depression screening tools amitriptyline 50 mg discount with visa. New perspectives into the molecular pathogenesis and treatment of kind 2 diabetes depression symptoms 7 year old buy 25 mg amitriptyline visa. Development of the medial hypothalamus: forming a useful hypothalamic-neurohypophyseal interface. Generation of neuropeptidergic hypothalamic neurons from human pluripotent stem cells. Alpha-melanocyte-stimulating hormone and N-acetyl-beta-endorphin immunoreactivities are 36. Effects of melatonin on neuronal activity within the rat suprachiasmatic nucleus in vitro. Molecular dissection of two distinct actions of melatonin on the suprachiasmatic circadian clock. Efficacy and safety of exogenous melatonin for secondary sleep disorders and sleep problems accompanying sleep restriction: meta-analysis. Clocks on high: the role of the circadian clock within the hypothalamic and pituitary regulation of endocrine physiology. The corticotropin-release inhibitory issue hypothesis: a evaluation of the proof for the existence of inhibitory in addition to stimulatory hypophysiotropic regulation of adrenocorticotropin secretion and biosynthesis. Thyrotropin-releasing hormone: function in the treatment of West syndrome and related epileptic encephalopathies. Feedback regulation of thyrotropin-releasing hormone gene expression by thyroid hormone in the hypothalamic paraventricular nucleus. Central regulation of hypothalamic-pituitarythyroid axis underneath physiological and pathophysiological circumstances. Changes in adrenal standing have an effect on hypothalamic thyrotropin-releasing hormone gene expression in parallel with corticotropin-releasing hormone. Evidence for thyrotropinreleasing hormone and glucocorticoid receptor-immunoreactive neurons in varied preoptic and hypothalamic nuclei of the male rat. Hippocampal input to the hypothalamus inhibits thyrotrophin and thyrotrophin-releasing hormone gene expression. Inhibition of hypothalamic thyrotropin-releasing hormone messenger ribonucleic acid during food deprivation. Leptin prevents fastinginduced suppression of prothyrotropin-releasing hormone messenger ribonucleic acid in neurons of the hypothalamic paraventricular nucleus. Transcriptional regulation of the thyrotropin-releasing hormone gene by leptin and melanocortin signaling. Dominant and recessive inheritance of morbid weight problems related to melanocortin 4 receptor deficiency. Human recombinant interleukin-1 beta decreases plasma thyroid hormone and thyroid stimulating hormone levels in rats. Interleukin-1 beta stimulates somatostatin biosynthesis in primary cultures of fetal rat brain. Impairment of hypothalamicpituitary-thyroid perform in rats handled with human recombinant tumor necrosis factor-alpha (cachectin). Intrinsic pituitary interleukin-1 beta is induced by bacterial lipopolysaccharide. Role of mineralocorticoid receptors on the hypothalamus-pituitary-adrenal axis in people. Opposing crosstalk between leptin and glucocorticoids rapidly modulates synaptic excitation by way of endocannabinoid release. Central mechanisms of stress integration: hierarchical circuitry controlling hypothalamopituitary-adrenocortical responsiveness. Circuits and mechanisms governing hypothalamic responses to stress: a story of two paradigms. Organization and regulation of paraventricular nucleus glutamate signaling systems: N-methyl-Daspartate receptors. Interleukin-1 stimulates the secretion of hypothalamic corticotropin-releasing issue. Corticotropin-releasing factor-producing neurons within the rat activated by interleukin-1. The neuroendocrine management of the innate immune system in health and brain diseases. Impaired diurnal adrenal rhythmicity restored by constant infusion of corticotropin-releasing hormone in corticotropin-releasing hormone-deficient mice. Characterisation of a development hormone-releasing issue from a human pancreatic islet tumour. Growth hormone-releasing factor from a human pancreatic tumor that caused acromegaly. Growth hormonereleasing hormone: construction, gene expression and molecular heterogeneity. Immunocytochemical demonstration of development hormone-releasing think about gastrointestinal and pancreatic endocrine tumors. Isolation and sequence analysis of the human corticotropin-releasing factor precursor gene. Identification of a novel murine receptor for corticotropin-releasing hormone expressed in the coronary heart. Urocortin 2-deficient mice exhibit gender-specific alterations in circadian hypothalamus-pituitaryadrenal axis and depressive-like conduct. Urocortin three regulates glucose-stimulated insulin secretion and power homeostasis. Corticotropin-releasing hormone antagonists, astressin B and antalarmin: differing profiles of activity in rhesus monkeys. Mouse mutants for the examine of corticotropin-releasing hormone receptor perform: development of novel treatment methods for temper problems. The organization of the stress system and its dysregulation in depressive illness. Expression of the rat growth hormonereleasing hormone gene in placenta is directed by an alternate promoter. Nonsense mutation within the human growth hormone-releasing hormone receptor causes progress failure analogous to the little (lit) mouse. Pathophysiology of the neuroregulation of progress hormone secretion in experimental animals and the human. The progress hormone response to hexarelin in patients with different hypothalamic-pituitary abnormalities.
Amitriptyline 25 mg buy online
Longitudinally oriented spinal tracts (white matter) encompass central areas (gray matter) where neuronal cell our bodies are located anxiety 10 year old generic 50 mg amitriptyline with visa. Sensory axons coming into the dorsal a part of the spinal twine originate in the dorsal root ganglia depression symptoms vs sadness amitriptyline 50 mg with visa, that are situated outside the spinal cord. Along with the motor axons originating from the central a half of the spinal cord, they leave the spinal segment via the intervertebral foramen at every segment. Furthermore, it is necessary to notice that the motor synapses between the primary and the second motoneurons are situated within the ventral a half of the grey matter (alpha-motoneuron), whereas the neuronal cell our bodies of the peripheral sensory neuron are situated in the dorsal root ganglion throughout the intervertebral foramen. While in the cervical backbone the C4 nerve root exits the C3/4 foramen, the L4 nerve root exits the L4/5 foramen in the lumbar spine. In the cervical spine, the cell bodies of the alpha-motoneuron are located roughly one degree greater than the exiting nerve root. This is of clinical relevance as focal injury to the anterior spinal cord can cause a more distal deficit than one would anticipate from the location [25]. Somatotopic group of the spinal cord Neurological Assessment in Spinal Disorders Chapter 11 295) the posterior column containing sensory nerve tracts conducting position sense (proprioception) and awareness of deep pressure) the ventrolateral column contains spinothalamic tracts for the feeling of ache and temperature) the posterior-lateral tract transmitting voluntary motor management through the pyramidal tract Classification A easy differentiation of neurological impairment is expounded to the trigger and onset of the issues and mainly distinguishes between:) traumatic injuries) non-traumatic disorders Spinal issues can additional be differentiated with regard to the affected neuronal constructions, i. Focal compression syndromes of the spinal cord in degenerative disorders are predominantly localized on the cervical and lumbar spinal level [3, 6, 92, 115]. Here, the spine has to cope with the very best biomechanical stress (a excessive range of movement and being beneath nice strain throughout daily activities) and is susceptible to develop a degenerative stenosis resulting either in cervical myelopathy or lumbar spinal canal stenosis and neurogenic claudication. Furthermore, the cervical spinal canal can show a congenitally lowered diameter with increased vulnerability to degeneration or even minimal cervical trauma with severe neurological sequelae [107, a hundred and fifteen, 130]. Spine tumors of various etiology (intra- or extradural) and dignity always need to be considered in patients assumed to undergo from spinal problems [1, 44, 66, 81]. Spinal hemorrhages predominantly occur acutely/spontaneously in sufferers present process anticoagulation treatment, or affected by tumors or arteriovenous malformations [37, 58, 83, ninety one, 114, 116, 126]. Specifically in instances with atypical presentation, disorders aside from these of the spinal wire should be considered within the differential diagnosis. Similarly, in older and multi-morbidity patients, peripheral nerve disorders can be confused with spinal wire problems and should be specifically addressed. In patients with a slowly growing polyneuritis, an rising motor weak point, reduction of strolling distance and occurring pain can mimic a lumbar spinal stenosis, whereas neurophysiological testing may be applied to distinguish between each issues. Focal compression syndromes predominantly happen in the cervical or lumbar backbone In atypical instances also think about non-spinal differential diagnosis 296 Section Patient Assessment Table 1. For example, the primary clinical symptom of a diabetic neuropathy can seem as a severe painful affection of the femoral nerve with a marked paralysis of the quadriceps muscle. This symptom can be easily confused with an L3 radiculopathy and the mismatch between an intensive medical image (weakness, loss of reflexes and sensory deficit) and usually appearing lumbar imaging should indicate a further work-up. Impairment or loss of motor and/or sensory operate in the cervical segments (C0�T1) is identified as tetraplegia. In accordance with the standard neurological classification of spinal cord harm. A additional differentiation is made with regard to the completeness of the lesion as:) complete) incomplete the distinction between complete and incomplete is predicated on the preservation of any sensory or motor operate inside the last sacral segments S4�S5. The preservation of lower sacral segments indicates an incomplete lesion 298 Section Patient Assessment Table 2. The medical examination may be complemented by extra neurophysiological research notably when the clinical examination is proscribed as a outcome of poor cooperation by the patient. The following clinical symptoms ought to be distinguished by the examiner:) motor weakness) sensory deficit) altered reflexes (cave: spinal shock)) ache syndromes) autonomic capabilities (bowel and bladder dysfunction) the examination can allocate the signs to neurological syndromes similar to:) radiculopathy) polyneuropathy) myelopathy) central paresis Neurological syndromes are non-specific for the underlying pathology However, neurological syndromes are non-specific with regard to their spinal cause. Pain Pain is essentially the most incessantly complained of symptom which might lead one to the impaired neurological structure [49, 95, 108]. The pathophysiology and diagnostic assessment of ache are lined in Chapters 5 and forty. Sensory Deficits Distinguish the sensory qualities (light contact, pin prick, proprioception) Although a number of sensory qualities (heat�cold, ache, touch, stress, static and dynamic two-point discrimination, vibration sensation) can be distinguished, the examination of:) mild touch) pinprick) proprioception Neurological Assessment in Spinal Disorders Chapter 11 299 is most regularly applied in clinical practice to assess spinal wire dysfunction [13, 41, fifty one, sixty two, eighty four, 89, ninety nine, 101]. While the light touch sensation assesses the perception of contact as utilized by the finger or cotton wool, the pinprick sensation identifies the flexibility to sense a pointy needle tip. The vibration sense is reliably tested with a tuning fork that permits totally different grades of vibration recognition to be distinguished [45, 86, ninety eight, 99]. It is essential to bear in mind that particularly incomplete lesions of the spinal twine can cause extra diffuse distributed sensory deficits whereas radicular and peripheral lesions result in circumscribed modifications. Patients with cervical myelopathy typically complain of ache, clumsiness and numbness of the entire arms and/or feet. In ischemic lesions of the central a part of the spinal wire, the predominant scientific discovering is an impairment of pain and temperature sensation. In such instances, sensation to contact remains preserved while pain and temperature sensation is abolished, which is usually distributed in a segmental pattern. The affection of the posterior column as induced by a B12 hypovitaminosis or hardly ever as a result of trauma causes a reduction of the vibration sense with predominant gait disturbance. Consider central lesions in diffuse/dissociated sensory deficits Motor Deficits the differentiation of the causes of muscle weak spot can generally trigger diagnostic difficulties. Radicular lesions are sometimes related to pain emanating into the respective dermatomes and present paresis of the innervated muscles. The differentiation between radicular and peripheral nerve lesion is usually troublesome (see below). A painless atrophy of hand or foot muscle at all times demands a neurological work-up and an extended differential analysis has to be thought-about:) amyotrophic lateral sclerosis) spinal muscular atrophy) myelopathy) neuropathy (hereditary motor neuropathies) Painless muscle atrophy calls for a detailed neurological differential analysis Reflex Deficits the scientific examination of higher and decrease limbs as properly as sacral reflexes is necessary in the evaluation of spinal issues. The Hoffmann and Tr�mner signs could be noticed in wholesome people with hyperexcitability and are solely pathologic if they happen unilaterally or in very pronounced trend. Polysynaptic reflexes a the absence of the anal reflex indicates a lesion at S3 � 5. After acute spinal cord harm, the bulbocavernosus reflex may be elicted inside 72 h even in spinal shock in contrast to the decrease limb tendon reflexes. Recovery of the bulbocavernosus reflex with out sensory or motor function indicates a whole spinal twine lesion. Gait Disorders Gait dysfunction must be detailed by questioning and clinical exams. Ataxic gait with increased danger of falls (impaired stability and skill for line walking), want for an enlarged assist base, and elevated problem in walking in darkness are indicators of disturbed proprioception. That could additionally be triggered (with decreasing frequency) by:) polyneuropathy) posterior column disorders) cerebellar lesion Gait disorders should be completely differentiated 302 Section Patient Assessment Several scientific checks can be utilized to distinguish between these disorders. In polyneuropathy the most specific discovering is a pattern of loss of reflexes and sensory deficit in a distal and sock like distribution (below the knee and/or in the space coated by socks) of impaired gentle touch sensation and reduction of proprioception. The latter is clinically examined by passively moving the foot or toes up and down and asking the blindfolded patient to describe the course of motion. This test is named after the German neurologist Moritz Heinrich Romberg (1795 � 1873). Maintaining stability whereas standing within the stationary place depends on intact sensory pathways, sensorimotor integration centers and motor pathways. The main sensory inputs are:) joint place sense (proprioception), carried within the dorsal columns of the spinal cord) imaginative and prescient Crucially, the brain can acquire sufficient data to preserve steadiness if both the visual or the proprioceptive inputs are intact. The first stage of the check (standing with the eyes open) demonstrates that no much less than one of many two sensory pathways is undamaged, and that sensorimotor integration and the motor pathway are intact.
Amitriptyline 25 mg cheap amex
Conditions aside from diabetes insipidus are the more widespread causes of hypernatremic encephalopathy depression definition us history amitriptyline 25 mg buy with visa. It could also be brought on by lack of hypotonic fluids by the kidney or the intestine or by insensible losses or could additionally be secondary to administration of hypertonic sodium-containing fluids or hyperalimentation depression test dysthymia amitriptyline 50 mg buy with mastercard. Studies indicate that within the mind so-called idiogenic osmoles are generated intracellularly, so the diploma of cell shrinkage is less than could be expected primarily based on the diploma of hypernatremia. These idiogenic osmoles belong to three natural classes: polyols, trimethylamines, and amino acids and their derivatives. This asynchrony will increase the potential for cerebral edema and worsening of the neurologic condition with overzealous treatment of hypernatremia. If the process is very long, one would possibly consider a low-dose vasopressin given repeatedly with fluid as described earlier for postoperative or trauma-induced hypothalamic/ neurohypophyseal diabetes insipidus. In nephrogenic diabetes insipidus there might be a higher emphasis on fluid substitute to keep away from dehydration and hypernatremia. It is necessary that such patients preserve therapy of all anterior and posterior pituitary deficiencies repeatedly as a end result of the balance among these replacements is essential. This finding led to the identification of the first well-described instances of this dysfunction in 1957245 and the following scientific investigations that resulted in delineation of the essential characteristics of the syndrome. PromotingaSalineDiuresis In sure scientific conditions, such as chemotherapy or use of some contrast agents, diuresis is desirable to minimize renal toxicity. If desmopressin is continued and a large volume of regular saline is given, natriuresis and hyponatremia will be induced. Withholding desmopressin and replacing fluids with 5% dextrose in water (D5W) may lead to hyperglycemia, whereas changing with normal saline might lead to hypernatremia. It has been reported that very low-dose vasopressin administered repeatedly intravenously (similar to that described earlier for comatose patients) can be utilized. Hypoosmolality and Hyponatremia Incidence Hypoosmolality is the most common dysfunction of fluid and electrolyte balance encountered in hospitalized patients. The incidence and prevalence of hypoosmolar issues rely upon the nature of the patient population studied as well as on the laboratory methods and standards used to diagnose hyponatremia. Most investigators have used the serum sodium concentration ([Na+]) to decide the clinical incidence of hypoosmolality. When hyponatremia is outlined as a serum [Na+] of lower than a hundred thirty five mEq/L, prevalences as excessive as 15% to 38% have been noticed in studies of both acutely and chronically hospitalized sufferers. Nonetheless, hyponatremia is necessary clinically because (1) extreme hypoosmolality (serum [Na+] levels <120 mEq/L) is associated with substantial morbidity and mortality rates251; (2) even comparatively mild hypoosmolality can shortly progress to more dangerous ranges in the course of the course of therapeutic management of other issues; (3) overly speedy correction of hyponatremia can itself trigger extreme neurologic morbidity and death252; and (4) it has been noticed that mortality charges are much larger, from 3-fold to 60-fold higher, in patients with even asymptomatic levels of hypoosmolality compared to normonatremic sufferers. Plasma osmolality can be decided directly by measuring the freezing-point depression or the vapor pressure of plasma. Direct measure and indirect calculation produce comparable outcomes under most conditions. Therefore, only the concentrations of effective solutes in plasma should be used to confirm whether clinically significant hyperosmolality or hypoosmolality is current. Sodium and its accompanying anions represent the main effective plasma solutes, so hyponatremia and hypoosmolality are often synonymous. The first is pseudohyponatremia, which is produced by marked elevations of either lipids or proteins in plasma. Measurement of serum [Na+] by ion-specific electrodes, which is now commonly employed by most medical laboratories, is less influenced by excessive concentrations of lipids or proteins than is measurement of serum [Na+] by flame photometry. However, this could still happen if the electrode measurement is done utilizing a diluted pattern of the serum. Once equilibrium between both fluid compartments is achieved, the total efficient osmolality remains relatively unchanged. This situation most commonly happens with hyperglycemia and represents a frequent cause of hyponatremia in hospitalized sufferers, accounting for up to 10% to 20% of all instances. This can be produced both by an extra of body water, leading to a dilution of remaining body solute, or by a depletion of physique solute, either Na+ or K+, relative to physique water. This classification is an oversimplification, as a end result of most hypoosmolar states involve vital components of both solute depletion and water retention. Body fluid losses by themselves rarely cause hypoosmolality because excreted or secreted body fluids are often isotonic or hypotonic relative to plasma and therefore tend to enhance plasma osmolality. Therefore, medical proof of hypovolemia strongly supports solute depletion as the cause of plasma hypoosmolality, however absence of clinically evident hypovolemia by no means fully eliminates this as a risk. This mechanism contributes to some instances of diuretic-induced hypoosmolality during which depletion of total physique K+ usually happens. Despite the importance of solute depletion in some patients, most cases of clinically vital hypoosmolality are attributable to increases in complete physique water somewhat than by main losses of extracellular solute. This can occur because of both impaired renal free water excretion or extreme free water consumption. The former accounts for most hypoosmolar problems because regular kidneys have enough diluting capability to allow excretion of 18 to 24 L/ day of free water. The renal mechanisms responsible for impairments in free water excretion can be subgrouped in accordance with whether or not the main impairment in free water excretion occurs in proximal or distal components of the nephron, or each. Any disorder that leads to a decrease in glomerular filtration price causes elevated reabsorption of each Na+ and water within the proximal tubule. As a outcome, the flexibility to excrete free water is limited because of decreased supply of tubular fluid to the distal nephron. Distal nephron impairments in free water excretion are characterised by an lack of ability to dilute tubular fluid maximally. These disorders are often related to abnormalities in the secretion of vasopressin. Just as depletion-induced hypoosmolar problems normally include an essential component of secondary impairments of free water excretion, most dilutioninduced hypoosmolar problems also involve important degrees of secondary solute depletion. Despite the appeal of this concept, its validity has by no means been demonstrated conclusively in both human or animal research. An different theory is that cell volume is maintained under hypoosmolar situations by extrusion of intracellular solutes such as potassium. Although latest studies of volume regulation throughout hyponatremia have centered on the mind, all cells regulate volume by cellular losses of both electrolyte and natural solutes to various degrees. Third, outcomes of animal studies in both dogs274 and rats275 have indicated that a major factor of chronic hyponatremia is attributable to secondary Na+ losses quite than water retention; the relative contributions from water retention versus sodium loss range with the length and severity of the hyponatremia: water retention was found to be the major reason for decreased serum [Na+] in the first 24 hours of induced hyponatremia in rats, but Na+ depletion then turned the predominant etiologic issue after longer intervals (7-14 days) of sustained hyponatremia, significantly at very low (<115 mEq/L) serum [Na+] ranges. Consequently, the degree to which hyponatremia is the results of dilution because of water retention versus solute depletion from quantity regulatory processes can range markedly, depending on which phase of adaptation the affected person is in and the relative charges at which the completely different compensatory processes happen. A excessive urine [Na+] signifies that renal causes of solute depletion are more likely. Therapy with thiazide diuretics is the most common cause of renal solute losses,259 particularly in the aged,277 however mineralocorticoid deficiency because of adrenal insufficiency or mineralocorticoid resistance must be thought of in addition to (less commonly) renal solute losses as a outcome of salt-wasting nephropathy. In these patients hypoosmolality results from an even greater expansion of total body water brought on by a marked discount in the rate of water excretion (and sometimes an increased rate of water ingestion). These sufferers typically have a low urine [Na+] due to secondary hyperaldosteronism.
Red Chickweed (Scarlet Pimpernel). Amitriptyline.
- Dosing considerations for Scarlet Pimpernel.
- Are there safety concerns?
- How does Scarlet Pimpernel work?
- What is Scarlet Pimpernel?
- Depression, liver disorders, herpes, cancer, kidney disorders, wounds, itching, painful joints, and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96391
Buy generic amitriptyline 50 mg online
The mechanism of unfavorable regulation is less well understood than ligand-dependent activation depression nutrition buy amitriptyline 25 mg fast delivery, and there could additionally be several mechanisms mood disorder with psychotic symptoms 50 mg amitriptyline cheap with mastercard. The magnitudes of activation and repression have been arbitrarily set at 10-fold for this theoretical example. In cells, these magnitudes range as a function of coactivator and corepressor concentration and in a goal gene�specific manner. This interaction results in redistribution of coactivators from the other transcription factors that positively regulate the gene. Recent proof strongly helps this model, whereby inhibition of the activity of the positively appearing components ends in the noticed negative regulation. Multiple signal-dependent kinases can phosphorylate nuclear receptors, leading to conformational modifications that regulate function. The properties of coactivators and corepressors are additionally regulated by phosphorylation. Its activity is ligand impartial but probably interacts with coactivators and will affect the magnitude of activation by agonists or partial agonists. Tissue Selectivity of Ligands Interacting With Nuclear Receptors Many endogenous hormones that act through nuclear receptors accomplish that in a tissue-specific method. The most obvious mechanism is differential expression of the receptors, both in house. A gamma-aminobutyric acid transporter driven by a proton pump is current in synaptic-like microvesicles of pancreatic beta cells. Pharmacology and signaling of prostaglandin receptors: a number of roles in irritation and immune modulation. The relationship between the insulin-binding capability of fat cells and the cellular response to insulin. Insulin resistance, insulin insensitivity, and insulin unresponsiveness: a necessary distinction. Historical evaluation: a short historical past and private retrospective of seven-transmembrane receptors. The nicotinic acetylcholine receptor: the founding father of the pentameric ligand-gated ion channel superfamily. Gating of pentameric ligand-gated ion channels: structural insights and ambiguities. Role of -arrestins and arrestin domaincontaining proteins in G protein-coupled receptor trafficking. Role of -arrestins and arrestin domain-containing proteins in G proteincoupled receptor trafficking. Beta-arrestin-dependent formation of beta2 adrenergic receptor-Src protein kinase complexes. Identifying ligandspecific signalling within biased responses: concentrate on opioid receptor ligands. Structural and practical homologies in the receptors for insulin and the insulin-like development elements. Structural congruency of ligand binding to the insulin and insulin/type 1 insulin-like growth factor hybrid receptors. An allosteric mechanism for activation of the kinase domain of epidermal progress issue receptor. Association of Sos Ras change protein with Grb2 is implicated in tyrosine kinase sign transduction and transformation. Membrane focusing on of the nucleotide trade factor Sos is sufficient for activating the Ras signaling pathway. Evidence for a useful function of Shc proteins in mitogenic signaling induced by insulin, insulin-like development factor-1, and epidermal progress factor. Identification of main tyrosine phosphorylation websites in the human insulin receptor substrate Gab-1 by insulin receptor kinase in vitro. Expression cloning of an activin receptor, a predicted transmembrane serine kinase. Betaglycan binds inhibin and can mediate functional antagonism of activin signalling. Myostatin signals by way of a reworking growth factor beta-like signaling pathway to block adipogenesis. Ligand-independent oligomerization of cell-surface erythropoietin receptor is mediated by seventy one. Diabetes mellitus: its differentiation into insulinsensitive and insulin-insensitive sorts. Postreceptor insulin resistance contributes to human dyslipidemia and hepatic steatosis. Activation of a member of the steroid-hormone receptor superfamily by peroxisome proliferators. Nuclear receptors and human disease: thyroid receptor beta peroxisome-proliferator-activated receptor gamma and orphan receptors. Vitamin D receptor mutations in patients with hereditary 1,25-dihydroxyvitamin D-resistant rickets. Structural overview of the nuclear receptor superfamily: insights into physiology and therapeutics. Structural analysis of nuclear receptors: from isolated domains to integral proteins. Direct repeats as selective response components for the thyroid-hormone, retinoic acid, and vitamin-D3 receptors. Cell- and gene-specific regulation of major target genes by the androgen receptor. A hierarchical community of transcription components governs androgen receptor-dependent prostate most cancers development. Hormone-dependent coactivator binding to a hydrophobic cleft on nuclear receptors. Ligand binding and co-activator meeting of the peroxisome proliferator-activated receptor-gamma. Nuclear receptor corepressors activate quite than suppress basal transcription of genes which might be negatively regulated by thyroid hormone. Thyroid hormone signaling in vivo requires a stability between coactivators and corepressors. Hormone-responsive enhanceractivity maps reveal predictive motifs, oblique repression, and targeting of closed chromatin. Transactivation features of the N-terminal domains of nuclear hormone receptors: protein folding and coactivator interactions. Multi-modulation of nuclear receptor coactivators by way of posttranslational modifications. Anatomical profiling of nuclear receptor expression reveals a hierarchical transcriptional community.
Amitriptyline 25 mg cheap with visa
If testosterone levels are elevated depression symptoms bipolar best 50 mg amitriptyline, subsequent conversion to estradiol might result depression pms quality 50 mg amitriptyline, resulting in gynecomastia, oily skin, and acne. This approach may be marginally more practical than remedy with gonadotropins and will trigger less gynecomastia. These approaches require sturdy affected person commitment, as sufficient spermatogenesis is probably not attained for 2 years or longer regardless of normalized testosterone ranges. Aliquots of successfully generated sperm samples ought to be frozen for future impregnation. Clomiphene citrate is a weak estrogen receptor antagonist that stimulates gonadotropin secretion in regular women and men. Clomiphene has been used to increase spermatogenesis in men with partial hypogonadotropism with oligospermia or azoospermia and regular to mildly low serum testosterone concentrations, significantly in men with useful hypogonadism, with variable outcomes. Although ovulation is commonly induced and pregnancy achieved by gonadotropin therapy, a high fee of a quantity of follicle development stays a priority. Thyroid-Stimulating Hormone Physiology the hypothalamic-pituitary-thyroid system performs a critical function in growth, progress, and cellular metabolism with thyroid hormone availability and motion managed by complicated mechanisms on the tissue stage. Thyrotroph cells comprise approximately 5% of the practical anterior pituitary cells and are situated predominantly within the anteromedial areas of the gland. They are smaller than the other cell sorts and are irregularly shaped with flattened nuclei and relatively small secretory granules ranging from one hundred twenty to 150 �m. The downstream promoter region (-200 and below) is required for placental expression, intermediate sequences are required for gonadotroph expression, and upstream promoter components are required for thyrotroph-specific expression. Tanycytes appear to be the primary contributor to the negative feedback regulation of the hypothalamic-pituitarythyroid axis. Secretion charges are enhanced as a lot as 15-fold in hypothyroidism and are suppressed in hyperthyroidism. L-Thyroxine is used for substitute remedy, and dosing variables are similar to those required for treating major hypothyroidism. The molecule is converted peripherally into the lively T3 and has a 7-day half-life with secure blood ranges. Thyroid hormone substitute accelerates cortisol metabolism and requirements and will due to this fact exacerbate primary hypoadrenalism or precipitate adrenal crisis in sufferers with perturbed adrenal operate. Craniofacial developmental anomalies, together with anencephaly, lead to cleft lip and palate, basal encephalocele, hypertelorism, and optic nerve hypoplasia with varying degrees of pituitary dysplasia and aplasia. If these infants survive, lifelong acceptable pituitary hormone alternative is required. Congenital basal encephalocele might end result in the pituitary herniating through the sphenoid sinus roof, leading to pituitary failure and diabetes insipidus. Patients heretofore recognized with idiopathic isolated or polyhormonal pituitary failure may in fact harbor a mutation, and because the transcriptional management of pituitary improvement is clarified, growing numbers of mutant genes have turn out to be apparent (see Table 8-2). The phenotype varies with both the kind of mutation as properly as the age of the patient. The hypogonadism appears to be a as a outcome of variable and combined hypothalamic and pituitary operate. Exogenous anabolic steroid and glucocorticoid remedy suppresses the reproductive and adrenal axes, respectively. Hypothyroidism, hypoadrenalism, or hypogonadism trigger hyperplasia of specific trophic cells due to lack of unfavorable feedback and generally actual pituitary tumor formation. In addition to pituitary apoplexy, different vascular accidents similar to aneurysms, strokes, cavernous sinus thrombosis, and arteritis can cause pituitary hormone insufficiency. Isolated hormone pituitary hormone deficiencies can also happen as a manifestation of vascular abnormalities together with arteritis or subarachnoid hemorrhage (Table 8-11). HeadTrauma the pituitary could also be partially or completely broken by birth trauma, cranial hemorrhage, fetal asphyxia, or breech supply. Head trauma may result in direct pituitary damage by a sella turcica fracture, pituitary stalk part, traumainduced vasospasm, or ischemic infarction following blunt trauma. Pituitary manipulation or injury throughout surgical procedure results in transient or permanent diabetes insipidus and ranging levels of anterior pituitary dysfunction. Hypopituitarism following head trauma normally manifests within a yr after the insult. Seventy-five p.c of sufferers with posttraumatic pituitary failure are young males under age 40 years involved in a motorized vehicle accident. Virtually all sufferers with subsequent pituitary failure have a history of lack of consciousness following trauma, and half of all such patients have documented cranium fracture. Diabetes insipidus is the most common endocrine disorder, encountered in about 30% of those patients. Patients might present with an isolated pituitary hormone deficiency or with combined hypothalamic-pituitary hormone deficiencies. Accompanying midline defects and eye abnormalities suggest involvement of developmental processes. Acquired Disorders In the absence of demonstrable hypothalamic-pituitary anatomic damage, and after excluding genetic and syndromic causes of pituitary insufficiencies, acquired, usually transient, causes of pituitary failure ought to be considered (see Table 8-5). Causes of pituitary insufficiency together with pituitary tumors, parasellar masses, hypophysitis, aneurysms, and pituitary apoplexy had been mentioned earlier. Note the contrast between the hypogonadal affected person (panel A, proper side) and his unaffected equivalent twin (left side). Magnetic resonance imaging confirmed a lobulated, contrast-enhancing suprasellar mass (coronal view in panel B [arrow] and sagittal view in panel C [arrow]). Images in medical drugs: hypogonadism because of pituicytoma in an similar twin. After a median dose of 5000 rads directed on the skull base, nasopharynx, or skull, as a lot as 75% of patients will develop pituitary insufficiency inside 10 years. Stereotactic radiosurgery directed to the pituitary gland additionally leads to 23% of sufferers exhibiting pituitary deficits inside forty eight to 96 months. Ideally, rigorous long-term screening ought to unmask incipient pituitary failure previous to onset of morbidity. An empty sella might develop as a consequence of a major congenital weak point of the diaphragm in those patients in whom no secondary trigger is clear. Up to 50% of patients with major empty sella have associated benign intracranial hypertension. Although an empty sella is usually an incidental discovering, if more than 90% of pituitary tissue is compressed or atrophied, pituitary failure usually happens. The spectrum of medical options of pituitary insufficiency is decided by several elements. In acquired pituitary insufficiency the medical spectrum relies upon upon the degree of hormone deficiency, the variety of hormones impaired, and the rapidity of onset. In congenital types, the sooner the age of onset, the larger the severity of thyroid, gonadal, adrenal, development, or water disturbances.
Cheap amitriptyline 50 mg on line
Many physicians and lay people think about circumcision routine depression hormones buy cheap amitriptyline 50 mg on-line, however complications depression testosterone levels order amitriptyline 50 mg line, although relatively uncommon, could be severe. Therefore, despite the perceived simplicity of the procedure, meticulous attention to anatomic landmarks, wound care, and follow-up is necessary. Abnormality of urethra or penile shaft (foreskin may be essential for later reconstruction [e. Lack of really "knowledgeable" parental consent (see Chapter 2) Circumcision of neonates has incessantly been used as a mannequin to study the response of the newborn to ache (see Chapter 6) (8) However, until lately, neonatal circumcision has been carried out with out anesthesia. Plastibell plastic cone (Hollister, Libertyville, Illinois); out there in presterilized packs; size range primarily based on dimension of glans penis: 1. Local anesthetic: 1% lidocaine hydrochloride without epinephrine in a tuberculin syringe with a 1. Although solely the two dorsal penile nerves are focused by the injection of lidocaine, the ventral penile nerve can be blocked by infiltration via the subcutaneous tissue. Some have advocated additional anesthesia ventrally, blocking the perineal nerves (a department of the pudendal nerve) b. Identify by palpation the symphysis pubis and corpora cavernosa at the penile base. Estimate depth of pubic bone from penile base to indicate necessary depth of injection (should not exceed zero. Pierce skin over certainly one of dorsal nerves at penile root, and advance fastidiously posteromedially (0. When Plastibell is used, parents ought to be told to name their doctor if ring has not fallen off within 10 days. Make positive that internal epithelium is completely separated from glans penis and that prepuce could be retracted to visualize entire circumference of coronal sulcus. Residual skin should retract completely, and the whole coronal sulcus have to be visible to keep away from postcircumcision adhesions, the most common complication. Technique A full description of formal surgical excision has been excluded from this version because of the requirement to use sutures and the related elevated danger of bleeding in contrast with strategies that involve crushing of tissue. Analgesia is usually obtained after 3 minutes and typically disappears within 20 to half-hour. Marking the place of the sulcus with ink on the pores and skin of the penile shaft, prior to the process, is helpful in demarcating this very important landmark. Grasp rim of prepuce on dorsal aspect with mosquito hemostats, roughly 2 to 4 mm aside. Place decrease blade of enormous, straight hemostat between prepuce and glans to within three to four mm of corona, ensuring to keep away from urethra. Use of circumcision clamp (1) Check clamp to ensure that all elements are current, match properly, and are in good working order. If the clamp is removed before 10 minutes has elapsed, wound edge hemostasis could also be insufficient. If significant bleeding occurs through the process, remove the gadget and seek for bleeding vessel-avoid blindly inserting sutures. Never use electrocautery; nonetheless, use of an ultrasound dissection scalpel has been described as a safe alternative to electrocautery (6). D: Grasping the prepuce with mosquito hemostats in preparation for the dorsal slit process. B: Placing the baseplate of the clamp over the stud till the stud engages with the baseplate (inset). Tissue beneath ligature will atrophy and separate from bell in 5 to 8 days (maximum 10 to 12 days). Management of Postoperative Bleeding Postoperative bleeding normally stems from inadequate hemostasis. Most are mild and respond to wet to dry dressings and Sitz baths, however fatalities have been reported a. Skin bridge between penile shaft and glans (commonly as a result of inadequate skin removing and failure to visualize the corona on follow-up examination) c. Urethral laceration during dorsal slit procedure (avoided by maintaining urethra in view at all times in the course of the procedure) b. Loss of penis (most commonly due to accidents related to cautery) (20) /amputation of glans (10,12) c. Cyanosis/necrosis of glans penis caused by overly tight Plastibell, misplaced sutures, or overtight circumferential bandage (7,13). Urethrocutaneous fistula associated with use of Gomco clamp or Plastibell (most generally triggered by utilizing a Plastibell or clamp of incorrect dimension or failure to acknowledge congenital megaloureter) (19) 5. Tight (or occlusive) dressing or glanular prolapse by way of ring of Plastibell (21) b. Chordee most commonly is the end result of dense ventral scarring from inflammation; could also be due to removing of extra skin from shaft or secondary to a skin bridge 9. Displacement with lodging of Plastibell round penile shaft or glans penis (9) thirteen. Excessive removing of pores and skin must be handled with utility of antiseptic (iodophor) every day and not with grafting or burying the penis in scrotum. Recurrence of pneumothorax (27) Reaction to epinephrine used to control bleeding a. Local vasospasm (may lead to necrosis of the glans) Complications because of local anesthetic a. Methemoglobinemia has been reported following exposure to prilocaine, procaine, benzocaine, and lidocaine (28). Neonatal genital herpes simplex sort 1 infection after Jewish ritual circumcision: fashionable medicine and religious custom. Postcircumcision necrosis of the glans penis: gray scale and shade Doppler sonographic findings. Use of buccal mucosa to simulate the coronal sulcus after traumatic penile amputation. Acute venous stasis and swelling of the lower abdomen and extremities in an toddler after circumcision. A localized collection of pus ensuing from bacterial organisms that trigger necrosis, liquefaction, accumulation of leukocytes and debris, which presents as a fluctuant gentle tissue swelling that will have related erythema and induration. In newborns, normally caused by invasion of native bacterial flora (2), direct inoculation. Gloves and gown Antiseptic swabs or cup containing antiseptic solution 1-mL syringe Nonbacteriostatic, isotonic saline without preservative 23-gauge needle 2- � 2-inch gauze squares Scalpel with no. To set up free drainage of contents from a superficial abscess Surgical incision and drainage is the definitive therapy for gentle tissue abscesses. Antibiotic therapy alone is ineffective in the setting of localized abscess (1,2,8�11) 2.
Amitriptyline 25 mg order without a prescription
Supportive care during neuroprotective hypothermia within the time period newborn: Adverse results and their prevention depression headaches amitriptyline 25 mg discount amex. A comparability of cooling methods used in therapeutic hypothermia for perinatal asphyxia bipolar depression explained amitriptyline 50 mg order on-line. Is cerebral blood flow/metabolic mismatch throughout rewarming a threat factor after profound hypothermic procedures in young children Elevated morphine concentrations in neonates handled with morphine and prolonged hypothermia for hypoxic ischemic encephalopathy. Therapeutic hypothermia changes the prognostic value of clinical evaluation of neonatal encephalopathy. Assessment of mind tissue injury after reasonable hypothermia in neonates with hypoxic-ischemic encephalopathy: a nested substudy of a randomised managed trial. Cerebral Resistance Index is much less predictive in hypothermia encephalopathic newborns. Consider surgical excision as a substitute for prevent the development of amputation neuromas (1,2) B. To prevent accidental avulsion of appendage if extra digit on a slender base were to turn out to be entangled, apply a gentle dressing or adhesive bandage till toddler is steady enough for removal. Clamp hemostat as close to the bottom of extra digit as potential however with out drawing up extra pores and skin. Using as a slicing information the sting of the hemostat farther from the hand, excise the digit. When extra digit is on radial side of hand or is a duplicated thumb 344 Removal of Skin Tags. If the lesions are massive or in critical areas, removal is best delayed beyond the neonatal interval. Removal of tags this massive requires surgical excision rather than ligation for best end result and may be associated with other malformations. Nonfunctional extra digit on ulnar facet of left hand (note wide base; surgical excision is preferred). A selective strategy to therapy of ulnar polydactyly: preventing painful neuroma and incomplete excision. Reconstruction of a congenital nasal deformity utilizing pores and skin tags as a chondrocutaneous composite graft. A: Place fantastic hemostat as near base of additional digit as possible, and firmly secure ligature between clamp and hand. B: After finger turns white, excise digit tag outside hemostat, leaving ligature in place for autoamputation of residual stump. Indications Newborn male circumcision, one of the oldest formally recorded surgical procedures, stays controversial (1�3). Simple linear�cruciate or elliptical skin incisions might lead to extra unpleasant scar formation (4). Bacteremia Premature incision could also be prevented by the use of ultrasound with or without diagnostic needle aspiration (19,20). Superficial abscess in the site of a Broviac central venous line insertion in the left anterior chest wall. Care must be taken in areas with plentiful vascular and neural structures, such as the groin, posterior knee, antecubital fossa, and neck (5). Prepare as for main process if abscess is to be drained, or for minor process if needle aspiration alone is to be carried out (see Chapter 5). Process aspirated material instantly: Gram stain and culture for anaerobic and aerobic organisms; Giemsa stain for suspected herpes. The dimension of the incision must be as small as potential yet enable for continued adequate drainage. Obtain specimen for culture with cotton-tipped applicator, if not obtained by prior aspiration with syringe and needle. Evacuate exudate from abscess with light strain from finger or hemostat wrapped in gauze. Use caution when probing abscess with finger in circumstances of suspected retained overseas bodies or fragments-for this cause, hemostat wrapped in gauze is the preferred methodology (4). If necessary, insert mosquito hemostat into abscess cavity and unfold blades to break septa and to launch remaining collections of pus. Randomized, doubleblind, placebo-controlled trial of cephalexin for treatment of uncomplicated skin abscesses in a inhabitants in danger for community-acquired methicillin-resistant Staphylococcus aureus infection. Communityacquired methicillin-resistant Staphylococcus aureus: an rising risk. Diagnostic worth of needle aspiration in Haemophilus influenzae sort b cellulitis. Role of microbiological investigations in the management of non-perineal cutaneous abscesses. Imaging of superficial soft-tissue infections: sonographic findings in instances of cellulitis and abscess. Hazards of piercing and facial body art: a report of three sufferers and literature review. Management and outcome of children with pores and skin and soft tissue abscesses caused by community- forty nine Sepideh Nassabeh-Montazami Phototherapy Phototherapy is the most common therapeutic intervention used for the therapy of hyperbilirubinemia (1). Phototherapy causes three reactions: configurational and structural isomerization of the bilirubin molecule and photo-oxidation, leading to polar, water-soluble photoproducts that could be excreted in bile and urine with out the need for conjugation or additional metabolism (2). The goal of phototherapy is to reduce serum bilirubin ranges to lower the chance of acute bilirubin encephalopathy and the more chronic sequel of bilirubin toxicity, kernicterus (1). Indications to begin phototherapy in infants with hyperbilirubinemia differ depending on gestational age, birthweight, hours of life, presence of hemolysis, and other danger factors corresponding to acidosis and sepsis (1,4). Preterm infants are at higher danger of growing hyperbilirubinemia in comparison with time period infants. Although guidelines have been proposed, the choice to provoke phototherapy in this group of infants remains variable and extremely individualized (4,6) (Table forty nine. Concomitant use of medication or agents that are photosensitizers can additionally be an absolute contraindication (8). Concurrent therapy with metalloporphyrin heme oxygenase inhibitors has been reported to end in gentle transient erythema (9). However, because the products of phototherapy are excreted in the bile, the presence of cholestasis might decrease the effectiveness of phototherapy. Bilirubin absorbs seen mild throughout the wavelength range of four hundred to 500 nm, with peak absorption at 460 � 10 nm thought of to be the simplest (2). Irradiance (intensity of light), expressed as watts per sq. centimeter (W/cm2), refers to the variety of photons received per sq. centimeter of exposed body floor space. Specific radiometers are generally beneficial for every phototherapy system, as a end result of measurements of irradiance may vary depending on the radiometer and the light source (1,10). A variety of phototherapy gear units exist and could also be free-standing, attached to a radiant warmer, wall-mounted, suspended from the ceiling, or fiberoptic systems. Congenital porphyria or a household historical past of porphyria is an absolute contraindication to the use of phototherapy. Management of hyperbilirubinemia in the new child toddler 35 or more weeks of gestation. The clinician is, due to this fact, confronted with an unlimited array of apparatus to choose from and must pay attention to benefits and drawbacks of every type.