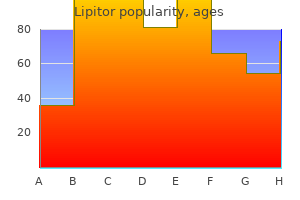
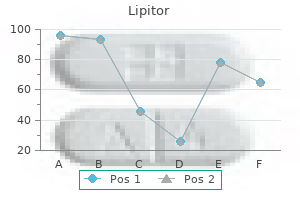
Lipitor dosages: 40 mg, 20 mg, 10 mg, 5 mg
Lipitor packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills, 240 pills
10 mg lipitor best
A set of retinal ganglion cells that reply in a linear style to luminance ranges project by way of the optic nerve and tract to the midbrain no cholesterol in eggs discount 5 mg lipitor overnight delivery. The decussation of approximately half of those fibers in the chiasm is one of the structural features responsible for the consensual response what should my cholesterol ratio be uk purchase 5 mg lipitor visa. The retinal axons terminate within the pretectum inside the olivary pretectal nucleus (sometimes simplified to pretectal nucleus), which in flip initiatives bilaterally to the Edinger-Westphal preganglionic nucleus, with the decussating fibers crossing in the posterior commissure. Parasympathetic fibers from the Edinger-Westphal preganglionic nucleus exit with the oculomotor nerve and terminate within the ipsilateral ciliary ganglion. The postganglionic fibers reach the iris, where they excite the pupillary constrictor muscle. Damage to these postganglionic fibers produces a tonic dilated pupil (Adie syndrome) in which the constrictor muscle is supersensitive to cholinergic drugs. Cerebral aqueduct Visual Motor Systems 427 the pupillary gentle pathway described earlier than is activated when light is transduced by rods and cones, initiating a synaptic cascade that ends in firing of action potentials by ganglion cells. Thus, when light is shined into the attention of a patient, not solely does it produce direct and consensual pupillary responses, however the affected person may even "see" the sunshine due to an intact retinogeniculostriate pathway. However, an alternate and clinically relevant process has recently been established. The gentle reflex may also be initiated by a class of ganglion cells which are immediately activated by light, without synaptic enter from photoreceptors. These melanopsincontaining ganglion cells have large cell our bodies and very giant dendritic fields. If the optic nerve is partially damaged (A), shining a light-weight into that eye will produce diminished direct and consensual responses (left), however each might be present when the undamaged side is illuminated (right). A whole lesion at A would produce a blind eye, which might induce neither a direct nor a consensual response when the eye is illuminated. If the lesion happens in the optic tract (B) or pretectum, neither response is misplaced, although the reflexes may be weaker. If the lesion happens within the oculomotor nucleus or nerve (C), both direct and consensual responses will be misplaced in the eye on the lesion side, however they will be current within the different eye. Inhibitory trigeminal projection to levator palpebae motor neurons is indicated by the open circle. Lesions might result in lack of the direct or consensual pupillary response or in uneven pupil size (anisocoria). A dilated, unresponsive (fixed) pupil (or pupils) within the unconscious sufferer of head trauma is a grave signal. For instance, it could indicate that a space-occupying lesion has compelled the parahippocampal gyrus or uncus over the sting of the tentorium (uncal herniation), compressing the third cranial nerve. The pupillary fibers are superficially situated in the oculomotor nerve and are particularly delicate to pressure. Disease of the retina, the optic nerve, or in some circumstances the optic chiasm may lead to asymmetry of the pupillary response; this is a relative afferent pupillary defect (also referred to as a Marcus Gunn pupil). To take a look at the direct and consensual responses, a penlight is directed just under the visible axis of first one eye and then the opposite. Because the penlight is quickly moved forwards and backwards between the 2 eyes, that is commonly referred to as the swinging-light or alternating-light check. The effects of lesions in the sympathetic pathways (Horner syndrome) have already been mentioned. Another syndrome, referred to as Argyll Robertson pupil, is present in circumstances of tabes dorsalis (central nervous system syphilis). This pattern of sparing indicates that the afferent and efferent limbs of the pupillary mild reflex must be intact. Greater levels of pleasure, together with want, result in dilation of the pupil by way of sympathetic activation. This truth was recognized to Elizabethan ladies, who used tincture of belladonna to dilate their eyes for beauty functions. Today, cholinergic blockers are used to dilate the pupils for ophthalmologic examination. Blinking and Other Lid Movements the delicate buildings of the eye are protected by the eyelids. Blinks, some of which occur in response to somatosensory stimulation, guarantee safety for the eye. The corneal blink reflex is used to assess trigeminal sensory and facial motor nerve perform, in addition to the integrity of the lid pathways by way of the lateral pons. Second-order trigeminal neurons project immediately and not directly to the facial nucleus to excite orbicularis oculi motor neurons, which produce lid closure. In addition, an inhibitory pathway suppresses the exercise of antagonist levator palpebrae motor neurons in the oculomotor nucleus. Blinks also occur at regular intervals (averaging 12 blinks/min) as automatically triggered movements that spread the tear film over the cornea. The constant dispersal of the tear movie produced Visual Motor Systems 429 by rhythmic blinks prevents corneal lesions and scarring. Blepharospasm is a disorder on this rhythmic habits that leads to bouts of high-frequency blinking, whereas parkinsonism produces a decreased blink rate. To hold out of the road of imaginative and prescient, the lids also transfer with the eyes during vertical eye actions. These movements are produced by actions of the levator palpebrae muscle, which works in live performance with the superior rectus. Levator motor neurons receive inputs from cells in and near the vertical gaze centers. Consequently, Bell palsy, by which the facial nerve is broken, typically by a herpetic an infection of the nerve, leads to a lack of the blink reflex on the affected facet however no ptosis or lack of vertical gaze�related lid actions. The tarsal muscular tissues assist hold the lids open, as indicated by the partial ptosis current in the Horner syndrome. Their sympathetic innervation suggests that they regulate lid position with respect to emotional state. Relaxation of the tarsal muscular tissues results in the sensation of "heavy lids," which indicators the final tone of the autonomic system as the brain prepares to relaxation. Three-dimensional location of human rectus pulleys by path inflections in secondary gaze position. The Edinger-Westphal nucleus: a historic, structural and practical perspective on a dichotomous terminology. Corticocortical networks and corticosubcortical loops for the upper management of eye movements. Neural control of vergence eye actions: convergence and divergence neurons in midbrain. Characteristics and functional identification of inhibitory burst neurons within the skilled monkey. Functional properties of neurons within the monkey superior colliculus: coupling of neural exercise with saccade onset. Kaufman the visceral motor system has two main subdivisions, sympathetic and parasympathetic.
Lipitor 40 mg buy generic on line
Midcoronal crosssection and cross-section by way of femoral neck of (a) a 40-year-old lady and (B) a 77-year-old lady cholesterol free foods recipes proven lipitor 20 mg, respectively ldl cholesterol chart canada lipitor 20 mg order mastercard. However, in the weightbearing inferior femoral neck both trabecular and cortical bone are preserved. To date, all research have been carried out in caucasian populations, and new knowledge are needed to delineate longitudinal changes in bone microarchitecture in different race and ethnic groups, as a number of cross-sectional research point out that variations in bone microarchitecture could contribute to variation in fracture rates seen among different race/ethnic groups. In human cortical bone from the femoral middiaphysis, the tensile and compressive strengths and elastic moduli decrease roughly 2% per decade after age 20. For example, the vertebral trabecular bone volume declines approximately 50% from ages 20�80, whereas vertebral trabecular biomechanical properties (compressive elastic modulus, final stress, and power to failure) decrease by approximately 75%�90%. In fact, femoral neck area, neck width, and neck axis length are all positively correlated (r2 = zero. Evidence for an necessary function of trabecular bone in femoral power is offered by a research of the microstructural failure mechanisms of the human proximal femur during a sideways fall impression, which confirmed that tissue-level failure begins in the trabecular bone. In the spine, compressive and bending loads are transferred from the intervertebral discs to adjoining vertebral our bodies. Therefore, age-related changes within the properties of the intervertebral disc, the vertebral centrum, and the vertebral shell can every affect the load-bearing capability of the vertebrae. In addition to a profound decline in trabecular bone quantity, the thickness of the outer shell decreases from roughly 400�500 �m (age 20�40), to 200�300 �m (age 70�80), and to 120�150 �m in osteoporotic people. This article outlined the important thing determinants of bone strength, focusing on the important thing function of bone morphology and microarchitecture. While initial cross-sectional research assist an necessary role for trabecular and cortical bone architecture in skeletal fragility, extra potential studies are needed to clarify the scientific utility of bone structure measurements in vivo. There is marked heterogeneity in bone construction, even at a single skeletal web site, and research is required to decide the underlying contributors to this wide range in bone dimension, form, and construction. In specific, there are few studies analyzing the genetic determinants of bone structure138; though that is likely to be an space of nice curiosity with the rising availability of noninvasive imaging modalities to assess bone structure. High-resolution computed tomography for medical imaging of bone microarchitecture. High-resolution peripheral quantitative computed tomography for the evaluation of bone power and construction: a evaluate by the canadian Bone Strength Working Group. Physical activity when younger supplies lifelong benefits to cortical bone dimension and power in males. The ability of three-dimensional structural indices to reflect mechanical aspects of trabecular bone. Heterogeneity of the skeleton: comparability of the trabecular microarchitecture of the backbone, the iliac crest, the femur, and the calcaneus. Normal vertebral body size and compressive energy: relations to age and to vertebral and iliac trabecular bone compressive strength. Evaluation of orthogonal mechanical properties and density of human trabecular bone from the major metaphyseal areas with materials testing and computed tomography. Iliac crest trabecular bone volume as predictor for vertebral compressive power, ash density and trabecular bone volume in regular individuals. Influence of vertical trabeculae on the compressive strength of the human vertebra. Physical traits affecting the tensile failure properties of compact bone. Decrease in canine proximal femoral final strength and stiffness as a end result of fatigue injury. Prediction of the power of the aged proximal femur by bone mineral density and quantitative ultrasound measurements of the heel and tibia. Mechanical power of the proximal femur as predicted from geometric and densitometric bone properties on the lower limb versus the distal radius. Mechanical strength of the thoracolumbar backbone within the elderly: prediction from in situ dual-energy X-ray absorptiometry, quantitative computed tomography (QcT), higher and lower limb peripheral QcT, and quantitative ultrasound. Subperiosteal expansion and cortical remodeling of the human femur and tibia with growing older. Sexual dimorphism in vertebral fragility is extra the outcomes of gender variations in age-related bone achieve than bone loss. Effects of gender, anthropometric variables, and growing older on the evolution of hip strength in men and women aged over 65. Population-based research of age and sex differences in bone volumetric density, size, geometry, and construction at different skeletal websites. Similarities and differences between sexes in regional loss of cortical and trabecular bone 2. Bone fragility: failure of periosteal apposition to compensate for elevated endocortical resorption in postmenopausal girls. Distribution of intracortical porosity in human midfemoral cortex by age and gender. Intracortical remodelling and porosity within the distal radius and autopsy femurs of women: a cross-sectional study. Differences in bone microarchitecture between postmenopausal chinese-american and white ladies. Differences in macroand microarchitecture of the appendicular skeleton in young chinese and white girls. Differences in skeletal microarchitecture and energy in african-american and white women. The relationship between the structural and orthogonal compressive properties of trabecular bone. Quantitative ultrasound of the calcaneus reflects the material properties of calcaneal trabecular bone. Measurement and significance of three-dimensional structure to the mechanical integrity of trabecular bone. Direct three-dimensional morphometric evaluation of human cancellous bone: microstructural data from spine, femur, iliac crest, and calcaneus. Modeling the mechanical behavior of vertebral trabecular bone: effects of age-related changes in microstructure. Biomechanical results of intraspecimen variations in trabecular architecture: a three-dimensional finite component examine. Biomechanical competence of vertebral trabecular bone in relation of ash density and age in regular individuals. Sex differences in age-related changes in vertebral body size, density and biomechanical competence in regular individuals. Prediction of vertebral body compressive fracture using quantitative computed tomography. The intravertebral distribution of bone density: correspondence to intervertebral disc well being and implications for vertebral energy. Impact direction from a fall influences the failure load of the proximal femur as much as age-related bone loss. Ultrasound and densitometry of the calcaneus correlate with the failure loads of cadaveric femurs.
Purchase lipitor 40 mg overnight delivery
These sufferers often expertise headache is the cholesterol in shrimp bad lipitor 10 mg order without a prescription, tinnitus due to cholesterol test uk nhs 20 mg lipitor buy mastercard venous turbulence ("pulsatile intracranial noise"), and visual deficits (up to blindness) as a result of papilledema (swelling of the optic disc). Treatment features a program of weight reduction, medication, and, if needed, shunting (lumboperitoneal) or surgical fenestration of the optic nerve sheath, which consists of creating a window within the sheath to relieve pressure on the optic nerve. Although intracranial stress could initially be elevated and the ventricles enlarged, the strain might wax and wane over time or even subside to a high-normal degree; however, the effects of the increased pressure stay. In some patients, the mix of a tough shuffling gait and dementia may mimic the medical picture in neurodegenerative circumstances such as Alzheimer and Parkinson diseases. A mild and electron microscopic and immunohistochemical examine of human arachnoid villi. Integration of the subarachnoid area and lymphatics: is it time to embrace a brand new concept of cerebrospinal fluid absorption The morphology of cerebrospinal fluid drainage pathways in human arachnoid granulations. Functional ultrastructure of cerebrospinal fluid drainage channels in human arachnoid villi. Haines Overview-107 Development of the Meninges-107 Overview of the Meninges-108 Dura Mater-109 Periosteal and Meningeal Dura-109 Dural Border Cell Layer-109 Blood Supply-110 Nerve Supply-110 Dural Infoldings and Sinuses-110 Compartments and Herniation Syndromes-111 Cranial Versus Spinal Dura-112 Arachnoid Mater-112 Arachnoid Barrier Cell Layer-112 Arachnoid Trabeculae and the Subarachnoid Space-113 Arachnoid Villi-113 Meningioma-114 Origins and Locations-114 General Histologic Features-114 Symptoms and Treatment-115 Meningeal Hemorrhages-116 Extradural and "Subdural" Hemorrhages-116 Hygroma-116 Pia Mater-116 Cisterns, Subarachnoid Hemorrhages, and Meningitis-118 maximum protection, they can be very unforgiving within the case of trauma or in a illness course of. For example, growth of a tumor creates a mass which will improve intracranial strain and compress or displace varied parts of the brain. The neurologic deficits that outcome depend on the placement of the mass, the rapidity with which it enlarges, and which components of the mind are broken. Collectively, these neural crest and mesodermal cells kind the primitive meninges (meninx primitiva). At this stage, no obvious areas (venous sinuses, subarachnoid space) are current in the meninges. As development progresses (45 to 60 days of gestation), the ectomeninx turns into more compact, and areas seem on this layer that correlate with the positions of the future venous sinuses. Concurrently, the endomeninx turns into extra reticulated, and the areas that seem in its internal half correspond to the subarachnoid spaces and cisterns of the adult. By the tip of the first trimester, the general plan of the meninges is established. This defect is brought on by a failure of the ectoderm (future skin) to completely pinch off from the neuroectoderm and the primitive meninges that envelop it. The ectomeninx around the mind is steady with the skeletogenous layer that varieties the skull. This relationship is maintained in the adult, in whom the dura is intimately adherent to the inner surface of the skull. In the spinal column, the ectomeninx can also be initially steady with the growing vertebrae. However, as development proceeds, the spinal ectomeninx dissociates from the vertebral our bodies. A layer of cells stays on the vertebrae to form the periosteum lining the vertebral canal, and the larger a part of the ectomeninx condenses to form the spinal dura. In the vertebral column, this space may be used for the administration of epidural anesthetics. For safety, the mind and spinal twine are every encased in a bony shell, enveloped by a fibrous coat, and delicately suspended inside a fluid compartment. In the dwelling state, the nervous system has a gelatinous consistency, however when handled with fixatives, it becomes firm and simple to handle. With the exception of the intervertebral foramina, through which the spinal nerves and their related vessels pass, and the foramina within the skull, which serve as conduits for arteries, veins, and cranial nerve roots, this bony encasement is complete. After the neural tube closes (A and B), cells from the neural crest and mesoderm (C, arrows) migrate to surround the neural tube and kind the primordia of the dura and of the arachnoid and pia (D). The fibroblasts of every meningeal layer are modified to serve a selected operate. Layers of the dura are shown in shades of grey, the arachnoid in shades of pink, and the pia in green. This time period can also be generally used in clinical drugs (as in leptomeningeal cysts and leptomeningitis). Consequently, the spinal and cerebral subarachnoid spaces are also immediately steady with one another on the foramen magnum. Fibroblasts of the periosteal dura are larger and slightly less elongated than other dural cells. This portion of the dura is adherent to the inner floor of the cranium, and its attachment is particularly tenacious alongside suture lines and in the cranial base. In distinction, the fibroblasts of the meningeal dura are more flattened and elongated, their nuclei are smaller, and their cytoplasm could also be darker than that of periosteal cells. Although cell junctions are rarely seen between dural fibroblasts, the large amounts of interlacing collagen in periosteal and meningeal parts of the dura give these layers of the meninges great power. The innermost part of the dura consists of flattened fibroblasts that have sinuous processes. The extracellular areas between the flattened cell processes of dural border cells comprise an amorphous substance but no collagen or elastic fibers. Cell junctions (desmosomes, gap junctions) are occasionally seen between dural border cells and cells of the underlying arachnoid. Because of its loose association, enlarged extracellular spaces, and lack of extracellular connective tissue fibrils, the dural border cell layer constitutes a aircraft of structural weak spot at the dura-arachnoid junction. This layer is externally continuous with the meningeal dura and internally steady with the arachnoid. Consequently, bleeding into this space of the meninges will likely disrupt and dissect open the dural border cell layer somewhat than invade the overlying dura or the underlying arachnoid. A space may be created at this interface by, for example, trauma, bleeding from traversing veins, or a pathologic course of. Blood Supply the arterial supply to the dura of the anterior cranial fossa originates from the cavernous portion of the internal carotid, the ethmoidal arteries (via the ethmoidal foramina), and branches of the ascending pharyngeal artery (via the foramen lacerum). The center meningeal artery serves the dura of the middle cranial fossa and may be compromised by skull fractures of the parietal bone or the squamous portion of the temporal bone, doubtlessly resulting in an epidural hematoma. It is a department of the maxillary artery and enters the cranium through the foramen spinosum. The accessory meningeal artery (via the foramen ovale) and small branches from the lacrimal artery (via the superior orbital fissure) also serve the dura of the center fossa. The dura of the posterior fossa is served by small meningeal branches of ascending pharyngeal and occipital arteries and by minute branches of the vertebral arteries. The spinal dura is served by branches of major arteries (such as vertebral, intercostal, and lumbosacral) which may be located close to the vertebral column. These small meningeal arteries enter the vertebral canal via the intervertebral foramina to serve the dura and adjoining buildings.
Lipitor 20 mg buy amex
The lateral cholesterol levels uk nhs 40 mg lipitor purchase free shipping, medial cholesterol lowering diet plan mayo clinic buy lipitor 20 mg free shipping, and inferior vestibular nuclei are present at this level, whereas the superior vestibular nucleus turns into prominent more rostrally. This structure is composed of vestibulocerebellar and cerebellovestibular fibers and along with the laterally adjacent restiform physique constitutes the inferior cerebellar peduncle. The rostral portions of the solitary tract and nucleus are situated anterior to the vestibular nuclei and consist of a core of primary sensory fibers (tract) surrounded by cell bodies (nucleus). A major part of the central tegmental tract contains fibers coursing from the pink nucleus of the midbrain to the inferior olive of the medulla (rubroolivary fibers). Cells of the superior olive obtain input from the anterior cochlear nucleus and ship their axons into the lateral lemniscus on both sides. Axons of the spinal trigeminal tract synapse in the spinal trigeminal nucleus, the cells of which project to the contralateral thalamus as anterior trigeminothalamic fibers. Although ache and temperature alerts from the contralateral facet of the physique are conveyed by anterolateral system fibers, a few of these axons end within the pontine reticular formation as spinoreticular fibers. After crossing, these fibers ascend to type the lateral lemniscus and convey auditory indicators to the midbrain. At this degree, the anterior part of the medial lemniscus (lumbosacral representation) shifts somewhat laterally, and its posterior portion (cervicothoracic representation) assumes a more medial location. On each side of the midline, the corticospinal fibers located in the pyramid of the medulla are, in the basilar pons, utterly surrounded by the basilar pontine nuclei. In turn, most of their axons cross the midline and enter the cerebellum by way of the middle cerebellar peduncle (brachium pontis) as pontocerebellar fibers. Midpontine Level pigmentosus pontis) and constitute the biggest single location of noradrenaline/norepinephrine-containing cells within the central nervous system. Axons arising within the nucleus ceruleus project to widespread targets all through the cerebral cortex, a lot of the diencephalon, limbic system, brainstem, cerebellar cortex and nuclei, and spinal wire. This extensive projection arises from a cell group containing solely about 15,000 cell our bodies, which signifies that these fibers department profusely. When the activity level of the neurons in this nucleus is low, a state of quiescence is promoted, as in sleep. During times of regular nonstress and nonsleep exercise, these neurons have an intermediate level of exercise. However, when the activity of nucleus ceruleus neurons fluctuates outside of levels which are correlated with regular life activities, the affected person could experience conduct issues that require medical or psychiatric intervention. Consequently, this section emphasizes solely the features that are new at midpontine ranges. Most auditory fibers are actually concentrated within the lateral lemniscus, and rostral parts of the superior olivary nucleus appear simply lateral to the central tegmental tract. Anterior spinocerebellar fibers migrate posteriorly and enter the cerebellum by coursing over the floor of the superior cerebellar peduncle. This cell group is steady with the basilar pontine nuclei, and its axons enter the cerebellum through the contralateral brachium pontis. These cells also share similar options and connections with neurons of the basilar pons. The principal sensory and motor trigeminal nuclei are positioned in the lateral tegmentum, and the mesencephalic tract and nucleus extend rostrally in the lateral wall of the central gray. Ceruleus neurons contain pigment (hence the alternative name nucleus Rostral Pontine Level the only cranial nerve buildings present in the pontine tegmentum at rostral levels are the mesencephalic nucleus and tract. Anterior to the mesencephalic tract and nucleus is the locus (nucleus) ceruleus; this noradrenergic cell group additionally extends into the caudal midbrain. The rubrospinal tract is shifted even more medially, and the lateral lemniscus is close to the posterolateral surface of the brainstem at this level. The anatomic orientation is flipped to illustrate inner constructions in a clinical orientation; the clinically important tracts and nuclei are proven on a T2-weighted magnetic resonance image at a comparable stage of the facial colliculus in the caudal pons. Reticular and Raphe Nuclei Much of the pontine tegmentum is occupied by the reticular formation. The magnocellular reticular nuclei of the pons are, from caudal to rostral, the gigantocellular reticular nucleus and the caudal and oral pontine reticular nuclei. The parvocellular area nuclei of the pons comprise a diffuse lateral reticular formation at caudal and midpontine levels and include the medial and lateral parabrachial nuclei at rostral ranges. The Pons and Cerebellum Internal genu of facial nerve Abducens nucleus Facial colliculus Superior salivatory nucleus Facial nucleus Tegmentum 179 inhibition of ache at medullary and spinal ranges. In the caudal third of the tegmental pons, this cell group is replaced by the nucleus raphes pontis, which extends somewhat past midpontine ranges. The extra caudal of the pontine raphe nuclei (magnus) project primarily to the spinal wire; the extra rostral (pontis, superior central) project primarily rostrally to innervate a wide range of forebrain targets. Although the main neurotransmitter associated with the pontine raphe nuclei is serotonin, there are some enkephalin-containing cells in the raphe magnus. The arrow signifies the overall somatic afferent and particular visceral afferent parts of the intermediate nerve; these fibers course caudally to enter the spinal trigeminal and solitary tract and nuclei, respectively. Paramedian branches distribute to medial areas of the basilar pons, together with corticospinal fibers and the exiting fibers of the abducens nerve. The lateral part of the basilar pons is served by short circumferential branches, and the whole tegmental space plus a wedge of the middle cerebellar peduncle receives blood by way of the lengthy circumferential branches. At caudal levels (levels of the facial colliculus), the lengthy circumferential provide is supplemented by branches of the anterior inferior cerebellar artery. Rostrally, beginning at about the level of the principal sensory and motor trigeminal nuclei, the blood supply to the pontine tegmentum is supplemented by branches of the superior cerebellar artery. Next to the medial lemniscus at caudal pontine ranges is the nucleus raphes magnus (the raphe magnus). Occlusion of the paramedial branches at this degree ends in an ipsilateral abducens nerve paralysis and a contralateral hemiparesis (the Foville syndrome) with a variable contralateral sensory loss reflecting numerous levels of damage to the medial lemniscus. If the lesion in the Foville syndrome extends posteriorly into the pontine tegmentum, the affected person may have further deficits, corresponding to an ipsilateral horizontal gaze paralysis, indicating harm to the medial portions of the pontine reticular formation. If the world of damage is shifted considerably laterally to embrace the root of the facial nerve along with corticospinal fibers, the patient has a contralateral hemiparesis and an ipsilateral paralysis of the facial muscular tissues (the Gubler or MillardGubler syndrome). At midpontine levels, occlusion of paramedial and brief circumferential branches ends in the syndrome of the midpontine base. The primary structures broken and their corresponding deficits are corticospinal fibers (contralateral hemiparesis), sensory and motor trigeminal roots (ipsilateral loss of ache and thermal sense and paralysis of the masticatory muscles), and fibers of the middle cerebellar peduncle (ataxia). Lesions throughout the pontine tegmentum may mix cranial nerve indicators and lengthy tract indicators. Internal to the granular layer, and forming the core of each folium, is a layer of subcortical white matter composed of all fibers arriving (afferents to the cortex) or leaving (efferents of the cortex) the cerebellar cortex. Axons of Purkinje cells pass by way of the subcortical white matter to end in the cerebellar and vestibular nuclei. The anatomic orientation is flipped to illustrate inner structures in a scientific orientation; the clinically important tracts and nuclei are shown on a T2-weighted magnetic resonance image at a comparable degree of the rostral pons. The mossy fibers originate from cells situated in lots of nuclei throughout the brainstem and spinal wire. Traversing the granular layer are climbing fibers, en route to the molecular layer, and Purkinje cell axons leaving the cortex. Cerebellar nuclear cells project to a wide range of cell teams throughout the neuraxis, primarily by way of the brachium conjunctivum.
Buy cheap lipitor 20 mg
Gating total cholesterol chart by age 20 mg lipitor purchase otc, Selectivity cholesterol crystal definition cheap lipitor 40 mg without a prescription, and the Structure of the Sodium Channel A rating of voltage-dependent sodium and calcium channels (NaV and CaV) are known to exist in people. Sodium ions enter NaV only to find the inside lined with aspartate-glutamate-lysine-alanine sequences. This process causes nerves to "go to sleep" when pressure is utilized for a very lengthy time. Slow inactivation also contributes to adaptation in the neocortex, in motor neurons, in neurons of the subthalamic nucleus, and in nociceptor cell bodies in the posterior (dorsal) root ganglion. The ion pore has 4 vestibules toward the skin floor (two of that are numbered 1 and a pair of in panels B and D) and eight vestibules towards the inside (labeled three and 4) that all join together on the transmembrane area to type the excessive field strength selectivity filter. This is the other of the standard stimulus, a depolarizing pulse of current that sends the membrane potential optimistic to the threshold voltage. Whereas details vary from cell to cell, the essential mechanism relates to the three states of the sodium channel: during the hyperpolarizing pulse, increasingly more sodium channels swap over from the inactive to the closed state. A extremely cellular sequence of amino acids with a optimistic cost acts because the voltage sensor, not just for NaV and CaV but in addition for voltage-dependent potassium channels. Negative membrane potentials transfer these gating costs towards the inside of the cell; depolarizations trigger these amino acids to transfer outward and to open the pores to ion circulate. Conversely, low levels of calcium improve membrane excitability, producing unwanted spontaneous activity in nerves which are ordinarily quiescent. Again, knowing that the sodium channel can exist in one of three conformations-closed, Abnormal ranges of calcium, magnesium, and hydrogen ions alter nerve exercise. Increased concentrations stabilize nerve membranes, resulting in fatigue, depression, anorexia, and constipation. Indeed, massive infusions of magnesium sulfate have lengthy been the accepted secure treatment for the life-threatening hypertension and seizures accompanying the eclampsia of pregnancy. Reduced levels of those ions improve excitability, causing tetany (a combination of tingling sensations and muscle spasms), mental irritability, and ultimately seizures. Metabolic or respiratory alkalosis exacerbates symptoms of low calcium or magnesium and might trigger overt signs in borderline or latent tetany, as will tapping of the facial nerve in front of the ear (Chvostek sign) or causing a quick interval of ischemia by inflation of a blood strain cuff (Trousseau sign). The mechanism by which divalent cations like calcium modify the excitability of nerves is refined and is closely related to the detailed structure of the membrane lipid bilayer. The explanation begins with the reality that the phospholipids and the oligosaccharide groups adorning membrane proteins have adverse floor expenses on the surface of the bilayer. These adverse surface costs are current in giant numbers and 50 Essential Concepts create a voltage drop of 30 mV throughout the previous couple of nanometers instantly above the cell surface. Being doubly charged, divalent cations bind tightly to the adverse floor costs, so excessive concentrations of divalent cations neutralize the anionic surface expenses, abolish the unfavorable floor potential, and shift the entire membrane potential onto the lipid inside of the bilayer. A transmembrane protein such as the voltage-dependent sodium channel would then experience a more unfavorable voltage and have a reduced tendency to open: the neuron becomes stabilized. Conversely, when the concentrations of calcium or magnesium fall, divalents go away the membrane floor and more anionic costs are exposed. The surface potential turns into extra adverse and assumes a higher fraction of the membrane potential. All three components act together to scale back the size constant of the nerve, inflicting the currents on the lively nodes of Ranvier to have less of an impact at the distant resting nodes. With enough destruction, the size fixed becomes lower than the internodal distance. Individual cells adapt to their specific capabilities by expressing sodium, calcium, potassium, and chloride channels drawn from scores of families and a large number of transcripts. The ensuing pore sieves ions by measurement, allowing only the smallest hydrated monovalent cations to move. Repolarizing the Neuron Use-Dependent Block and the Treatment of Epilepsy Seizures are excessive and paroxysmal neuronal exercise, both regionally in a small area of the brain or spreading across the complete cortex. As a consequence, native anesthetic block of sodium channels is use dependent-the more the channel is used, the more channels are plugged, and the extra full the block is. No extra entry is possible once the channel is closed, however the local anesthetics can exit, releasing the block during times of inactivity. Toxins also interfere with sodium channel function, most famously tetrodotoxin (from the puffer fish and a North American salamander) and saxitoxin (from diatoms that trigger the red tide). Scorpion stings trigger ache, spasms, and finally paralysis as a outcome of their venom slows NaV inactivation and causes activation to occur at extra adverse voltages. Second, the loss of the electrical insulation of the myelin implies that the capacitance of the internode will increase and the resistance of the internode decreases. More often the duty is performed by a quantity of of the ten voltage-dependent calcium channels (CaV), that are plentiful all through the nervous system and various in their nature. A barely larger stimulus (3) brings the voltage above the threshold, causing a regenerative growth of the action potential. A superthreshold stimulus (4) causes the action potential to rise more quickly and to a higher amplitude as a end result of the sodium channels open sooner at extra optimistic potentials. B, the underlying sodium and potassium currents are both plotted as upward deflections. The open arrow factors to the time when the sodium current turns into larger in magnitude than the potassium present, permitting the motion potential to begin its regenerative part. Simply changing the membrane potential by the motion of a number of of the membrane channels might have extremely complicated penalties. Whereas hyperpolarization of a membrane would appear to move the neuron away from its threshold, the alternative may very well be the case, as mentioned in the anode break section. The experiment in this determine is one by which the neuron is first conditioned with a brief hyperpolarization and then tested with a depolarizing stimulus. Shown here is the crystallographic structure of a channel that could possibly be a homotetramer of and subunits. The T1 section of the subunit extends into the cytoplasm to join with the subunit, by way of which the complicated is controlled by cytoplasmic signals. The 4 subunit pairs that make up the channel are color coded and shown from the facet (A) and from above (C). S5 and S6 helices twine together to type the pore; the S1, S2, S3, and S4 helices hang out into the bilayer and sense the voltage. B, Increasingly fast excitatory inputs summate over time to yield bigger and larger stimuli to the neuron. A dozen channel varieties are involved within the specifics, with 4 NaV and CaV channels contributing to the spike activity. For instance, as synaptic input increases in frequency, the resulting changes in membrane potential start to add collectively and thus turn out to be more effective than anybody single postsynaptic potential; that is known as temporal summation. Similarly, as increasingly excitatory synaptic inputs turn into lively, the cell physique is depolarized to a greater and larger extent; that is referred to as spatial summation. Structure of complement poly-C9 decided in projection by cryo-electron microscopy and single particle evaluation. Role of tetrodotoxin-resistant Na+ current gradual inactivation in adaptation of motion potential firing in small-diameter dorsal root ganglion neurons. Water permeation across organic membranes: mechanism and dynamics of aquaporin-1 and GlpF. Epithelial sodium channel/degenerin family of ion channels: a variety of features for a shared structure.
Syndromes
- Uses 2 - 3 words (other than Mama or Dada) at 12 - 15 months
- Yellow skin
- Macrocephaly (abnormally large head size)
- X-ray of the affected area
- You feel short of breath or have chest pain
- Having light-colored skin, blue or green eyes, or blond or red hair
Lipitor 40 mg generic online
There is a large divergence in the finest way many agents produce their results foods not good cholesterol cheap lipitor 5 mg free shipping, which could be noticed at different organizational levels cholesterol found in shrimp 5 mg lipitor discount mastercard. Since bone turnover events characterize a sequence of various organic activities, intermittent, brief, or continuous delivery of the identical agent might give distinct skeletal responses. Skeletal responses to pharmacologic brokers could diminish with time as tolerance develops. One probable issue responsible for totally different drug doses inflicting various biological responses is the differential action of medication on the modeling and turnover stages. For example, a very small dose of 1,25-dihydroxy vitamin D3 reverses the endochondral progress abnormality associated with vitamin D deficiency, but excessive doses can produce markedly elevated osteoid within the metaphysis. It is necessary to acknowledge that skeletal cell-to-cell and cell-to-matrix interactions contain both bone cells and cells of the bone marrow and are managed by each systemic and native elements. Therefore, cell useful actions and cellular interactions represent the final widespread pathway of poisonous action quite than a basic mechanism of toxic action. Local events are influenced by circulating agents corresponding to hormones, however the results of circulating agents are additionally determined by local factors such as mechanical utilization. Certain ailments seem to affect one bone envelope (periosteal, Haversian, endosteal) more than others. In general, the endosteal bone envelope is more reactive and responsive than the Haversian envelope as a end result of endosteal (endocortical and trabecular) bone possesses a higher cumulative surface area, has cells with larger metabolic exercise, and experiences higher bone turnover. The surface-to-volume ratio and turnover fee is thrice higher in trabecular bone than cortical bone in both people and canine. In the rapidly rising young rat, the endocortical floor of the metaphysis is predominantly formative, whereas the periosteal metaphyseal surface is predominantly resorptive as the diameter of the bone is progressively lowered from extensive on the physis to relatively slim at the diaphysis. Certain drugs additionally seem to affect particular envelopes, and there are species variations as well. Mice handled with estrogens produce rather more marrow cancellous bone than do other animals. Bone loss following ovariectomy in rats and nonhuman primates is way larger than in dogs. It is nicely recognized that fracture therapeutic is much less vigorous in old animals than in young individuals; the identical is true in regards to the response of the skeleton to circulating toxicants. The modeling and turnover processes current beneath the expansion plates of rising animals reply to xenobiotics to a larger extent than do those in cortical or cancellous bone of older animals. In persistent research, drug toxicity might affect (or be influenced by) the incidence and severity of spontaneous lesions occurring in the animal strain being used. For example, persistent studies with nitrofurazone present a drug-related impact that tremendously increases the distribution and severity of age-related degenerative cartilage changes in rats. In the context of drug safety danger assessment, you will need to remember that many test article-related results on the rising physis represent on-target pharmacology and may not be related to human safety. Decisions regarding the relevance of such knowledge depend upon the proposed indication, exposure margin, and skeletal maturity of the supposed population of human patients. Decreased longitudinal bone growth is a typical finding in toxicity studies performed in quickly growing young rodents and could additionally be secondary to decreased food consumption (inanition) or occur as a consequence of test article activity. There are two primary categories of disruption to endochondral ossification: physeal dysplasia and physeal dystrophy. While physeal dysplasia and physeal dystrophy reflect very different toxicologic mechanisms, both result in functional impairment of the physis and decreased bone production and impaired growth. Hypertrophic pulmonary osteopathy (in this case, from a dog) results in in depth new bone formation beneath the periosteum in long bones. Krook, College of Veterinary Medicine, Cornell University; reproduced from Fundamentals of Toxicologic Pathology, second ed. Any substance able to interrupting the transition from hypertrophic cartilage to the calcified cartilage spicules of primary spongiosa, whether by inhibition of angiogenesis, lowered vascular penetration, chondrocyte cell dying, or a mixture of those processes, can cause physeal dysplasia. Distal femoral development plates are generally extra severely affected than proximal tibial plates, as depicted right here (C). Transverse fractures by way of the widened (and weak) dysplastic physis can happen through any cartilage zone. When publicity to these inhibitors ceases, these findings normally resolve to a outstanding diploma briefly order, although some slight residual chondrocyte column disorganization could persist. The final manifestation of decreased physeal thickness is physeal closure, which occurs prematurely if the situation develops is manifested in younger animals. Trabeculae of bisphosphonate-treated bone may have barely undulating surfaces associated with these enlarged osteoclasts, which may replicate the inability of the osteoclast to produce a resorption cavity of regular (more deeply scalloped) size. Cathepsin K inhibitors produce direct antiresorptive results on osteoclast function. Cathepsin K, an intracellular enzyme that digests type I collagen, is extremely expressed in osteoclasts as a means of degrading demineralized bone matrix. Bone resorption is decreased to a similar degree as with bisphosphonates, but bone formation is enhanced as a result of osteoclast crosstalk to osteoblasts stays intact. Retained major spongiosa and increased trabecular bone are morphologic features of bones from cathepsin-K deficient mice. Conversely, Wnt inhibition decreases ossification, resulting in reduced trabecular bone formation in the metaphysis of rising animals. Misplaced bone removing ends in trabecular splitting and a paradoxical enhance in trabecular connectivity in the face of decreased trabecular bone quantity by this ultimately catabolic course of. Decreased numbers of osteoclasts subjacent to the zone of hypertrophic chondrocytes impair the conventional elimination of extraneous calcified cartilage spicules. Primary and secondary spongiosa trabeculae numbers are elevated, resulting in a markedly elevated trabecular bone quantity within the metaphysis. Bisphosphonates are quickly incorporated into calcified cartilage and mineralized bone, rendering these extracellular onerous tissues resistant to acid digestion by osteoclasts. Exposure to bisphosphonates causes attribute changes to osteoclasts and erosion surfaces. Osteoclasts are Decreased Osteoblast Formation/Function At excessive doses, first technology bisphosphonate compounds, together with etidronate and clodronate, impair osteoblast operate as well as osteoclast function, resulting in extraordinarily low or successfully no bone turnover. Osteoid space and quantity are augmented (increased osteoid), indicating a mineralization defect. Administration of such brokers to young but skeletally mature dogs has been demonstrated to alter the structural integrity of the ribs and vertebral processes, leading to a number of spontaneous fractures. Such will increase could divert these stem cells toward adipocyte differentiation and away from osteoblast differentiation. Increased adiposity of bone marrow with reduced bone formation occurs because of this shift. The ensuing decreases in trabecular and cortical bone volume in the mouse could be dramatic. Many osteoclasts are located in lacunae on trabecular surfaces (arrows) that are regular areas, however different osteoclasts (arrowhead) are present in lacunae within the trabecular bone. As famous above, many inhibitors of chondrocyte proliferation, such as glucocorticoids, additionally inhibit osteoblast function. If these inhibitors have a relatively short half-life in comparability with the dosing interval. With respect to homeostatic bone transforming, the decreased bone formation results in a internet bone loss because the regular state of bone resorption followed by equal bone formation is now not in balance.
Buy lipitor 40 mg on line
At spinal ranges cholesterol levels over 1000 order 5 mg lipitor mastercard, the reticulospinal fibers are uncrossed and the fastigiospinal fibers are crossed cholesterol examples discount lipitor 20 mg with visa. Because their function is to assist preserve posture, these fibers tend to excite extensor motor neurons and inhibit flexor motor neurons. Raphespinal fibers originate mainly from the nucleus raphe magnus of the brainstem, descend bilaterally in posterior areas of the lateral funiculus, and function to modulate the transmission of nociceptive data at spinal ranges. Lesions within the brainstem or cervical spinal twine that interrupt these fibers end in ipsilateral ptosis, miosis, anhidrosis, and enophthalmos (Horner syndrome). Reticulospinal fibers in this area arise in the pontine reticular formation of the Spinal Cord 151 the brainstem, whereas vestibulospinal fibers originate from the vestibular nuclei. Lateral vestibulospinal fibers arise from the lateral vestibular nucleus, and medial vestibulospinal fibers originate primarily from the medial vestibular nucleus. Reticulospinal and vestibulospinal fibers of the anterior funiculus perform in postural mechanisms by way of their basic excitation of extensor motor neurons and inhibition of flexor motor neurons. Fibers of the anterior corticospinal tract are uncrossed, but most of these fibers cross in the ventral white commissure earlier than terminating on medial motor neurons that innervate axial muscle tissue. Tectospinal and vestibulospinal fibers are found only at cervical levels; the other fibers extend to decrease wire ranges. The comparatively simple construction of the spinal twine significantly misrepresents its useful importance. Although the wire is smaller in diameter than the little finger, descending motor control of the physique under the neck and all sensory enter from the same areas should traverse it. Consequently, small lesions in the spinal twine that might be thought of of little consequence in larger parts of the brain may cause international deficits or dying. As the twine merges into the brainstem, the organization and function of the central nervous system become progressively more advanced. Syringomyelia is commonly seen in sufferers with Chiari malformations in the posterior fossa but may be a consequence of trauma to the spinal wire, tumors, and infections, the signs are extremely variable but most regularly embody loss of ache and temperature sensations, extremity weakness, and unsteady gait. It is suitable at this point to contact on some basic options that correlate primarily with the structure of the spinal wire. Consequently, a lesion of this construction will harm fibers coursing in both instructions, leading to a bilateral lack of ache and thermal sensations that correlate with the broken ranges of the spinal cord. For example, if the lesion is in mid to low cervical levels, the pain and thermal sensory deficits will fall over the shoulders and arm in a "cape distribution. Because these lesions are often within the cervical ranges, extension of the syrinx into one anterior horn results in an ipsilateral weak point of the upper extremity; if both anterior horns are concerned, the weak point is bilateral. This is typically known as a noncommunicating syringomyelia to differentiate it from a cystic structure that may join with the central canal (communicating syringomyelia). On the opposite hand, a cavitation of the central canal is called a Injury to excessive cervical levels of the spinal twine is, in general, a catastrophic occasion. The phrenic nucleus is located in the central areas of the anterior horn at ranges C3 to C6. This cell group innervates the diaphragm and in excessive cervical lesions is disconnected from the facilities of the medulla that control respiratory. Consequently, in patients with excessive cervical lesions, preservation of the power to breathe turns into a main factor in care. Acute Central Cervical Spinal Cord Syndrome Syringomyelia the acute central cervical spinal wire syndrome, commonly called the central wire syndrome, is an incomplete spinal twine harm. [newline]This may end result from hyperextension of the neck (sometimes in a patient with bone spurs on the vertebrae) that momentarily occludes blood provide to the twine by way of the anterior spinal artery. Consequently, the deficits replicate the territory served by the branches of this vessel. The outcomes are bilateral weak point of the extremities (more so of the upper than of the lower), various levels and patterns of ache and thermal sensation loss, and bladder dysfunction. In general, function of the decrease extremities returns first, bladder perform next, and performance of the upper extremities final. For example, a spinal wire hemisection at T8 would have an result on the physique under that stage but would spare the higher trunk and higher extremity. A lesion involving the posterior columns bilaterally would lead to proprioceptive and discriminative touch losses below the extent of the lesion but would spare ache and thermal sensations. In our examine of methods neurobiology, we will explore these and different examples of dysfunction ensuing from spinal cord lesions. Organization within the Spinal Cord: the Anatomy and Physiology of Identified Neurons. Spinothalamic and spinohypothalamic tract neurons in the cervical enlargement of rats: I. Spinal wire: cytoarchitectural, dendroarchitectural, and myeloarchitectural group. The pain system, the neural basis of nociceptive transmission within the mammalian nervous system. Spinomesencephalic tract: projections from the lumbosacral spinal twine of the rat, cat, and monkey. For instance, the central areas of the medulla contain the cranial nerve nuclei affiliated with the medulla. This medullary area is rostrally continuous with the pontine tegmentum, which incorporates the cranial nerve nuclei associated with the pons. The basilar pons is bulbous and fairly attribute of the anterior facet of the pons. The pontine tegmentum contains parts of the trigeminal nuclei and the vestibular nuclei and, just rostral to the pons-medulla junction, the facial motor nucleus, superior salivatory nucleus, and abducens nucleus. These are the inferior cerebellar peduncle, the center cerebellar peduncle (or brachium pontis), and the superior cerebellar peduncle (or brachium conjunctivum), connecting the cerebellum to the medulla oblongata, basilar pons, and midbrain, respectively. Pons the term brainstem (sometimes written brain stem) can imply both the portion of the brain that consists of the medulla oblongata, pons, and midbrain or the portion that consists of these structures plus the diencephalon. For our purposes, due to this fact, the brainstem consists of the rhombencephalon, comprising the myelencephalon and metencephalon (but excluding the cerebellum), and the mesencephalon. These areas of the brainstem share a fundamental group, which is the topic of this chapter. The medulla is barely cone shaped and enlarges in diameter as it extends rostrally from the medulla�spinal wire junction toward the pons-medulla junction. The nuclei of the hypoglossal, vagal, and glossopharyngeal nerves in addition to portions of the nuclei of the trigeminal nerve are located in the medulla. The exit of the trochlear nerve is regarded as the pontomesencephalic junction on the posterior facet of the brainstem; along with its decussating fibers, it composes the isthmus rhombencephali (the transitional zone from pons to midbrain). In C, the cerebellum is removed to expose the posterior surface of the brainstem and the fourth ventricle. The posterior aspect of the midbrain is characterised by the superior and inferior colliculi, and their respective nuclei, and the anterior side by the crus cerebri and interpeduncular fossa.
Purchase 20 mg lipitor mastercard
The scientific deficits that result from a cerebellar lesion depend primarily on which of the three principal zones is involved; consequently cholesterol how to lower 40 mg lipitor buy free shipping, the three-zone terminology is used in this chapter cholesterol test to buy lipitor 5 mg generic otc. The lateral (hemisphere) zone occupies by far the largest a half of the cerebellar cortex. The fastigial (medial cerebellar) nucleus lies immediately adjoining to the midline and is functionally associated to the overlying medial zone of the cerebellar cortex. Lateral to the fastigial nucleus are the two interposed nuclei: the globose (posterior interposed) nucleus and the emboliform (anterior interposed) nucleus. These nuclei are functionally related to the overlying intermediate zone of the cortex. Lateral to the emboliform nucleus is the dentate (lateral cerebellar) nucleus, which seems as a large, undulating sheet of cells shaped like a partially crumpled paper bag. The lobules of the hemisphere are designated by the prefix H, to show which lobule of the hemisphere is steady with its corresponding (designated by the Roman numeral) vermal lobule. This nucleus is functionally related to the overlying lateral zone of the cortex; its giant dimension correlates with the massive size of this cortical zone. Most of the signals that depart the cerebellum achieve this via axons that arise within the cerebellar nuclei; the remainder journey on fibers that originate in the cerebellar cortex. Collectively, axons that come up in the cerebellar nuclei represent cerebellar efferent projections. These axons originate from cells in the cerebellar nuclei and generally use one of many excitatory neurotransmitters, glutamate or aspartate, and thus function to activate their targets. The fastigial nuclei usually project bilaterally to the brainstem via the juxtarestiform our bodies. Some neurons in every cerebellar nucleus ship axons or axon collaterals into the overlying cortical zone, where they terminate in the granular layer as mossy fibers. These axons are referred to as nucleocortical fibers, they usually exert an excitatory influence on the cerebellar cortex. Each Purkinje cell offers rise to an elaborate dendritic tree that radiates into the molecular layer. The "trunk" of the tree is a single main dendrite, which provides rise to a quantity of secondary dendrites, which in turn branch into many tertiary dendrites. Smooth branchlets emerge from secondary and tertiary dendrites, whereas spiny branchlets (covered by minute constructions known as gemmules) come up mainly from tertiary dendrites. In rostral views (A and E, J), the folia of the anterior lobe can characteristically be followed throughout the midline. The tonsil and its close relationship with the medulla are seen in inferior views (B and G, H); the peduncles and the lobes are clearly evident in anterior (ventral) views (C and H, I). Purkinje cell axons arise from the basal facet of its pear-shaped cell body and may give rise to recurrent collaterals. These axons traverse the granular layer and the subcortical white matter to eventually terminate in either the cerebellar or the vestibular nuclei. Purkinje cells projecting into the cerebellar nuclei (as cerebellar corticonuclear fibers) arise from all areas of the cortex, whereas those projecting into the vestibular nuclei (as cerebellar corticovestibular fibers) originate primarily from components of the vermis and the flocculonodular lobe. The common areas of cortex and nuclei served by the cerebellar arteries are additionally indicated on the left. Roman numerals indicate lobules of the vermis; numerals preceded by H indicate the corresponding lobules of the hemisphere. Granule Cell Layer There are three main types of neuron cell bodies throughout the granule layer. These are granular cells, which are terribly numerous and located in all areas of the cerebellar cortex; Golgi cells, which are bigger and also widely distributed; and unipolar brush cells, which are small neurons which have a restricted geographic distribution within the cortex. Their axons ascend into the molecular layer, the place they bifurcate to type parallel fibers. As indicated by their name, parallel fibers run parallel to the long axis of the folium. They also synapse with the cells intrinsic to the molecular layer, corresponding to basket and stellate cells. Granule cells use glutamate (or perhaps aspartate) as their neurotransmitter and thus have an excitatory impact on their goal cells. In reality, the granule cells are the primary excitatory neurons of the cerebellar cortex. The unipolar brush cell can also be excitatory but is found in strikingly fewer numbers and is restricted in its distribution within the cortex. All of the other neurons of the cerebellar cortex, as we will see, are inhibitory. Dendrites of Golgi cells department in the granular layer but lengthen primarily into the molecular layer without regard to plane of orientation. The third neuronal kind discovered throughout the granule layer is the unipolar brush cell. This dendritic process ends in a brush-like configuration made up of a cluster of dendrioles. Unipolar brush cells use glutamate as their neurotransmitter and are subsequently excitatory to their targets. The classic cerebellar glomerulus is a synaptic complicated found throughout all parts of the cerebellar cortex inside the granular layer. Note the construction of the cerebellar glomerulus (lower left) and the interplay of parallel and climbing fibers (upper right) with the dendritic processes of Purkinje cells. The mossy fiber rosette is centrally positioned within the glomerulus and types synapses with several granule cell dendrites. Golgi cell axons contact granule cell dendrites in the glomerulus, and the entire complex is encapsulated by astrocyte cell processes. Within the flocculonodular lobe and some adjoining cortical areas, there are lots of cerebellar glomeruli of the traditional arrangement described above. Because unipolar brush cells and their synaptic interactions are situated primarily in the flocculonodular lobe and vermis and because these cells obtain vestibular inputs, their function is most likely to be associated to cerebellar (and vestibular) control of eye movements, vestibuloocular reflexes, and various postural mechanisms mediated through efferent connections of the vestibular and reticular nuclei. The Purkinje cells are proven in sagittal (A, note the beaded appearance of the dendrites) and transverse (B, note the various parallel fibers) planes. Dendrites of Golgi cells (D) department into molecular and granular layers, whereas their axons (D, beaded structures) ramify in solely the granular layer. At the ultrastructural level (F), the Purkinje cell dendrite is surrounded by the numerous small profiles of parallel fibers. Stellate cells are often found in outer areas of the molecular layer and are incessantly referred to as superficial or outer stellate cells. The basket cell axon travels in the sagittal aircraft and gives rise to descending branches that kind elaborate "baskets" around the Purkinje cell physique.
Lipitor 5 mg purchase line
Centrally cholesterol treatment lipitor 10 mg generic overnight delivery, many of the fibers conveying ache and thermal sense coalesce to type the spinal trigeminal tract and terminate within the medially adjacent spinal trigeminal nucleus cholesterol levels blood lipitor 40 mg buy low cost. Other fibers conveying discriminative touch will synapse within the principal sensory nucleus; these fibers conveying proprioceptive data from the masticatory and extraocular muscular tissues and the periodontal ligament form the mesencephalic tract. In this latter situation, the first sensory cell our bodies kind the instantly adjacent mesencephalic nucleus. The blood provide to the brainstem originates from branches of the vertebral and basilar arteries. As we will see in the subsequent three chapters, branches of the vertebrobasilar system serve not only the medulla, pons, and many of the midbrain but additionally the complete cerebellum. In this respect, there are quite a few clinical events which will arise by which harm to the brainstem causes deficits that may vary from mild to severe or may trigger dying, in some cases all of a sudden. At this level, we briefly consider 4 herniation syndromes which are particularly related to the brainstem. In the case of the central nervous system, the causes of herniation are often related to a rise in intracranial strain (mass lesion-tumor; edema-brain swelling; large infarcts). Initially, there could also be a change in respiration, eye actions are irregular, and the pupils could additionally be moderately dilated. This is a critical neurologic event, and quick measures should be taken to lower intracranial strain. Uncal herniation initially compresses the midbrain, but if unchecked, the injury may prolong into lower brainstem ranges. Early signs embody a dilated pupil and irregular eye movements (oculomotor nerve involvement) with double vision ipsilateral to the herniation, adopted by weakness of the extremities (corticospinal fiber involvement) opposite to the dilated pupil. The end result may be occlusion of branches of the superior cerebellar artery with resultant infarction of cerebellar structures or obstruction of the cerebral aqueduct and hydrocephalus. The latter is seen as signs attribute of a rise in intracranial stress (vomiting, headache, lethargy, decreased levels of consciousness). This might lead to speedy compression of the medulla with a probably catastrophic neurologic consequence. The medulla is broken by mechanical compression or distortion, and the vessels serving the medulla are simultaneously compressed and occluded. This vascular insult ends in infarction of important respiratory and cardiac facilities in the medulla; there may be a rapid lack of respiration and a failure of medullary cardiac activity. This scientific event, if speedy, could represent a medical emergency and necessitate quick intervention. On the other hand, the tonsil could also be discovered within the foramen magnum as part of a developmental sequence and go largely undetected for considerable time. Caudal to the obex, the hypoglossal and dorsal motor vagal nuclei are small and are discovered in the central gray surrounding the central canal. Alar plate neuroblasts caudal to the obex give rise to the gracile and cuneate nuclei. Rostral to the obex, some alar plate cells migrate ventromedially to type the nuclei of the inferior olivary advanced. Concurrent with these developmental events, ascending and descending fibers are traversing the medulla. The medulla oblongata, or myelencephalon, is probably the most caudal segment of the brainstem. The cavity of the medulla consists of a narrow, caudal part, which is the continuation of the central canal of the cervical spinal cord, and a flared, rostral portion, which is the medullary a part of the fourth ventricle. Also, the medullary reticular formation incorporates cell teams that influence heart rate and respiration. The pyramids problem from the basilar pons and extend caudally to the motor (pyramidal) decussation, where about 90% of their fibers cross the midline. The basal and alar plates give rise to particular nuclei, and the surrounding mantle layer is invaded by axons originating from other levels. Beginning in the medulla, however, the essential derivatives of the primitive neural tube are augmented by the appearance of different constructions that characterize every brainstem level. Within the brainstem the basal and alar plates (cell columns) type discontinuous cell columns. Caudal rootlets of the vagus have been incorrectly called the medullary, or bulbar, root of the accessory nerve. In actuality, the accessory nerve is made up of axons that come up from cells within the higher levels of the cervical spinal cord (C1 to C5), ascend by way of the foramen magnum, coalesce to kind the accent nerve, after which exit the skull via the jugular foramen along with the glossopharyngeal and vagus nerves. Large tumors instantly exterior to this foramen may also involve the hypoglossal nerve root. The common area of the exit of the facial and vestibulocochlear nerves is clinically thought to be the cerebellopontine angle. Indeed, a vestibular schwannoma (incorrectly referred to as an acoustic neuroma) is a tumor of the vestibular portion of the eighth cranial nerve and is a lesion situated at the cerebellopontine angle. Rostral to the obex, these trigeminal fibers are located inner to a progressively enlarging restiform body. Rostrolateral to the gracile and cuneate tubercles and forming a prominent elevation on the posterolateral side of the medulla is the restiform body. This construction accommodates quite lots of afferent cerebellar fibers and turns into progressively larger because it extends towards the pons-medulla junction. In the caudal pons, fibers of the restiform physique be part of with a much smaller bundle, the juxtarestiform physique, to form the inferior cerebellar peduncle. The exceptions are the portion of the choroid plexus that extends out of the foramen of Luschka and the adjacent cochlear nuclei; these are served by branches of the anterior inferior cerebellar artery, a branch of the basilar artery. Caudal to the obex, the posterior medulla is served by the posterior spinal artery. Cranial nerves are indicated by Roman numerals, and the cerebellum has been removed from B and C. The vascular territory of the anterior spinal artery encompasses the medial lemniscus, hypoglossal root, and corticospinal fibers in the pyramid. Consequently, lesions of this vascular region lead to somatosensory and motor deficits reflecting harm to these buildings. Spinocerebellar axons enter the cerebellum through the restiform physique (posterior tract) or the superior cerebellar peduncle (anterior tract). Other ascending bundles, corresponding to spinoolivary and spinovestibular fibers, terminate within the medulla. At this level, the medial longitudinal fasciculus contains solely descending fibers. The majority of these descending axons influence, both instantly or indirectly through interneurons, the discharge patterns of motor neurons in the spinal wire grey matter. The spinal cord grey matter is replaced by the motor decussation (crossing of corticospinal fibers); the central grey matter enlarges; the posterolateral tract (dorsolateral fasciculus) and substantia gelatinosa of the spinal twine merge, respectively, into the spinal trigeminal tract and nucleus; and nuclei characteristic of the medulla seem. The caudal medulla is described within the following sections starting on the levels of the motor and sensory decussations. Because the gracile and cuneate fasciculi are collectively referred to as the posterior (or dorsal) columns, their respective nuclei are incessantly referred to as the posterior column nuclei.
Generic lipitor 5 mg free shipping
The deficit skilled by the affected person might range from decreased listening to to complete deafness in the affected ear lowering cholesterol tlc diet lipitor 20 mg generic mastercard. Depending on the trigger cholesterol test results chart lipitor 5 mg cheap visa, conduction deafness could resolve with treatment or by elimination of the obstruction. Resonance options of the pinna and meatus improve some frequencies greater than others in a direction-dependent style. For example, sounds coming toward the back of the head are baffled compared with those coming towards the facet of the head. Monaural (single-ear) localization is dependent upon such cues, and accuracy in localizing sound is impaired by injury to the pinna. Sounds are transmitted throughout the house from the tympanic membrane to the fluid-filled inside ear by a series of three bony ossicles: the malleus, incus, and stapes. On one finish of this chain, the arm of the malleus is hooked up to the tympanic membrane, and on the other end, the footplate of the stapes matches into the oval window on the interface with the fluid-filled vestibule of the inside ear. The three bones act as levers to cut back the magnitude of movements of the tympanic membrane while rising their force on the oval window. In this fashion, air pressure waves hanging the tympanic membrane result in plunger-like actions of the stapes against the oval window which have the mandatory drive to produce fluid stress waves in the cochlea. Its major components embrace a labyrinth of fluid-filled canals, specialised sensory epithelium of the organ of Corti, and neurons of the spiral ganglion with their peripheral and central axonal branches. The canals of the osseous and membranous labyrinth of the cochlea spiral two- and two-third turns from base to apex over a size of 34 mm. Uncoiled, the outer canals of the osseous labyrinth resemble a U-shaped tube and thus basically are one canal. Scala tympani, the lower chamber in cross part, is steady with the upper chamber at a hair pin curve, the helicotrema, on the apex of the cochlea. The fluid with which the vestibule and scala vestibuli and tympani are stuffed is perilymph. It contains the membranous labyrinth and at its base is connected by ductus reuniens to the saccule of the vestibular membranous labyrinth. The basilar membrane, extending from the spiral osseous lamina of the modiolus (as from threads of a screw) to the spiral ligament on the outer wall of the canal, is the lower boundary separating the scala media from scala tympani below. The endolymph, which fills the cochlear duct, is elaborated by the cells and rich capillary bed of the stria vascularis. The blue and red traces represent the spiral course of scala vestibuli and scala tympani, respectively, from base to apex of the cochlea. C, the basilar membrane features to separate waves of various frequencies within a sound. This membrane is slender and stiff at its base and becomes wider and extra versatile toward the apex, and the hair cell stereocilia improve correspondingly in top. These features "tune" the membrane so that every frequency of sound within the audible vary will trigger a wave in the basilar membrane that has its peak amplitude at a novel spot (near the base for high frequencies and near the apex for low frequencies). At this spot, the hair cells are excited most intensely, producing a peak in neural output. Note that the designation lateral or medial olivocochlear efferents refers to their origin within the superior olive, to not their goal within the organ of Corti. It consists of inner and outer hair cells, supporting cells, and the tectorial membrane. This tunnel is formed by the filamentous arches of the inside and outer pillar cells and is full of fluid just like perilymph. It is unsure how lots of the internal (about 3500) or outer (about 12,000) hair cells should be misplaced to disease, trauma, or growing older earlier than a just-noticeable sensorineural listening to loss ensues. The taller stereocilia in every hair bundle are involved with or embedded within the tectorial membrane. Consequently, motion of the basilar membrane and the organ of Corti will bend the stereocilia against the tectorial membrane and cause a graded depolarization of the hair cells. At their apical surface and hair bundle, internal 310 Systems Neurobiology hair cells are bathed in endolymph. Endolymph, like intracellular fluid, has a excessive concentration of potassium and low concentration of sodium ions. At the basilar membrane inner hair cells oppose the perilymph-filled scala tympani. In contrast to endolymph, perilymph, like cerebrospinal fluid, has a excessive focus of sodium and low concentration of potassium ions. This endolymphatic potential appears to be because of the selective secretion and absorption of ions by the stria vascularis. As the basilar membrane moves up in response to fluid movement within the scala tympani, the taller stereocilia are displaced towards the tectorial membrane. Damage to the stria vascularis leads to lack of the endolymphatic potential and failure of mechanoelectrical transduction. The transmitter causes depolarization of the afferent fiber, and an action potential is transmitted alongside the cochlear nerve fiber. The stimulus-related changes within the electrical potential between the perilymph and the hair cells could be recorded wherever in the cochlea. Electrocochleography measures patterns of fluctuation of electrical potentials in the cochlea to monitor results of internal ear fluid adjustments or of surgical procedure on cochlear function. In patients with profound sensorineural hearing loss, some audible sensation may be regained with cochlear implants having a selection of fantastic wire electrodes. Each wire is tuned to a broad frequency band from an electrical receiver, and the wires are implanted so that every stimulates nerve terminals at the appropriate tonotopic level alongside the cochlear spiral. Primary Afferent Innervation and Function Tuning of the Cochlea the cochlea acts as a frequency filter to separate and analyze individual frequencies from complicated sounds. The plunger-like motion of the stapes in the oval window compresses the perilymph. The basilar membrane is stiffest at its base and turns into progressively extra flexible toward its tip. The response of hair cells to the tone is strongest at the level of best displacement. Therefore the position from base to apex alongside the spiral of the basilar membrane and organ of Corti is directly associated to the frequency of the tone that will elicit a response. This relationship of frequency and cochlear position is the idea for the place principle of cochlear tuning. The cochleotopic order and thus tonotopic representation are highly conserved all through the auditory pathways. When outer hair cells depolarize, changes in conformation of lateral membrane proteins result in adjustments in the top of the cells and stiffness of their stereocilia.